Book Review: Which Country Has The World's Best Health Care?
I.
If you’re like me, all you’ve heard about international health care systems is “America sucks and should feel bad, everyone else is probably fine or whatever”. Is there more we can learn?
Our guide to this question will be Which Country Has The World’s Best Health Care , by Dr. Ezekiel Emanuel. Emanuel is a professor of bioethics, but I’ve been told to be less reflexively hostile to bioethicists. He got in trouble a few years ago for a comment that got summed up as “life after 75 is not worth living”, but he never used those exact words, and his point about the dangers of excessive life-prolonging medical care is well-taken. He opposes euthanasia, which I interpret as demanding state-sponsored coercive violence to prevent torture victims from escaping, but I know other people interpret it differently. And he’s the brother of former Chicago mayor Rahm Emanuel, but … nope, can’t think of any extenuating circumstances for this one.
Still, Emanuel is one of a very few people qualified to compare international health systems. And he claims additional expertise at ranking things, saying:
Which country has the world’s best health system? This is the type of question I usually love. I rank everything. I rank the 10 best meals I’ve ever had (#1 Alinea in Chicago, #2 Tanja Grandits in Basel, and #3 OCD in Tel Aviv). I rank chocolates (#1 Askinosie, #2 Dick Taylor of California, and #3 Fruition of New York. I rank Alpine cheeses (#1 is a tie between Alpha Tolman and Alp Blossom). I rank colleges. I rank academic departments of bioethics and health policy that compete with my own. I rank the meals I cook, the races I run, the bike rides I take, the speeches I give.
So: which country has the world’s best health care?
Emanuel hates having to give a clear answer to that question, but when confronted with the fact that he’s writing a book with that title and can’t really weasel out, he grudgingly admits that “the top tier would include Germany, the Netherlands, Norway, and Taiwan”.
He backs this up with ~300 pages of details about the health care systems of 11 major countries. I have to admit, I found this tough reading. Partly this is because health economics is an inherently boring topic. Partly it’s because national systems are a hodgepodge of historically contingent decisions that don’t really resolve into a single gestalt. And partly it’s because many countries run their medical systems entirely based on three-letter acronyms (did you know PBR financing in the NHS is partly under QOF schemes like BPTs that modify CCGs’ GMS contracts with PCNs?)
But partly it’s because all national health systems are surprisingly similar. One of my favorite books is David Friedman’s Legal Systems Very Different From Ours , which catalogues the world’s weirdest legal systems and expands your space of possibilities about what law codes would be like. I was hoping to find something similar here, but Emanuel’s book could easily have been titled Medical Systems Very Similar To Ours. People talk about how the US system is “privatized” and the Canadian system “socialized”, but a lot of this comes down to whether your payments for the same basic package are marked “paycheck deductions” vs. “taxes”. Or whether your choices are limited to one state insurance company vs. to 2-3 plans offered by your employer which are legally mandated to be basically the same. It was hard to find any really fundamentally different visions. And absent truly different designs, the 300 pages were a lot of stuff on how various bureaucracies were organized and which three-letter acronyms they used.
But after a valiant effort, Emanuel managed to distinguish five general types of health care system (Table 12-2 on page 364).
1: Socialized Medicine, where the government runs everyone’s insurance and most hospitals and clinics, ie it’s the main employer for doctors and other health professionals. Of the 11 countries studied, only the UK does this in general, although the Veterans Affairs system does it at a smaller scale in the US.
2: Single Payer With Very Limited Private Insurance is typical of Canada, China, Norway, and Taiwan. The government runs everyone’s insurance. But doctors, hospitals, etc can be independent businesses or nonprofits. They negotiate some kind of payment rate with the national insurance, who reimburses them. This is similar to how Medicare works in the US.
3: Single Payer With Substantial Private Insurance is typical of Australia and France. It works as above, except that citizens can buy private insurance which purports to be better than the standard government insurance in some way. For example, in Australia sometimes the private insurance has shorter waiting times, or can get you nicer rooms in more luxurious hospitals. Often the same doctors and hospitals treat the government and private patients, but give the private patients more time and resources, which leads to resentment and scandals. On the other hand, the private patients sometimes subsidize the public ones - ie a hospital charges extra for private patients and uses that to make up a funding shortfall if the government doesn’t pay them enough.
4: Single Payer Channeled Through Private Insurance is typical of Germany and the Netherlands. I think this is kind of like how charter schools work in the US: the government pays 100% of your costs, but you get to choose which insurance company (out of various heavily-regulated and basically identical plans) to go with. Then the insurance company pays private doctors and hospitals as usual.
5: Individuals Purchase Private Insurance **** is typical of the US and Switzerland. Individuals use their own money to buy insurance from private companies, which may be ambiguously-for-profit-but-heavily-regulated (some US companies) or not-for-profit (other US companies, Switzerland). If someone can’t afford to do this, they might get government subsidies (Switzerland) or get shunted to Medicaid / be out of luck (US). Those private insurances negotiate rates with private doctors and hospitals as normal.
How do the various systems compare?
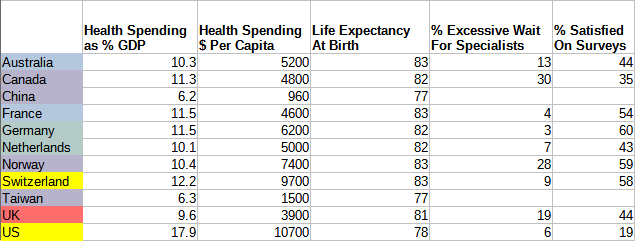 Source: page 370 of WCHWBS and the Commonwealth Fund. Things look a bit different depending on which statistics you chose to highlight; I did my best to be representative but you should double-check. Red countries are fully socialized, yellow ones are more privatized, various shades of blue are various types of single-payer.
Source: page 370 of WCHWBS and the Commonwealth Fund. Things look a bit different depending on which statistics you chose to highlight; I did my best to be representative but you should double-check. Red countries are fully socialized, yellow ones are more privatized, various shades of blue are various types of single-payer.
The only truly socialist health system here, that of the UK, looks maybe a little worse than average. It has the third-lowest satisfaction, the third-longest wait times, and the fourth-lowest life expectancy. Emanuel’s more thorough look agrees that the UK underperforms. But it’s also very cheap - the cheapest western health system on the list. Emanuel thinks the UK is probably close to the cost-quality Pareto frontier and not making any stupid mistakes, but has made the political decision to not fund its health system very much.
The typical American concern that single-payer-without-private-insurance systems have long wait times seems basically borne out. The two such systems we have good data for - Canada and Norway - are the two with the worst wait times on the list. Emanuel doesn’t think this is a necessary feature of those systems: he blames Canada’s wait times on their bad decision to give hospitals a constant amount of funding regardless of patient load, and says other single-payer systems that avoid this have limited waits. Single payer systems that involve private insurance in any way seem to do basically fine here.
(I’m ignoring China and Taiwan here for two reasons. First, they’re significantly poorer/less developed than the other countries on this list. Second, Taiwan works its doctors incredibly hard - they see about 2-3x as many patients per day as in other countries, for less money, and I’m not sure why they stay in medicine or how they stay sane. Third, China also underpays its doctors, and they compensate by being corrupt and demanding bribes before treating patients. All of these things make it hard to compare them to Western countries.)
The two countries with mostly private systems - Switzerland and the US - are also the two most expensive systems (though see here for a contrarian take on this). But the similarity ends there; Switzerland’s system has one of the highest patient satisfaction ratings, but America has the lowest. When I asked Swiss people about this, they said everyone in Switzerland is rich, which rescues a lot of otherwise-unsustainable systems. Certainly rich people in America get good health care. So maybe Switzerland isn’t as different as the numbers make it look, and these kinds of systems are just bad.
Single-payer implemented through private insurance - Germany and the Netherlands - comes out looking pretty good: these are 2 of the 4 countries Emanuel puts in his top tier. I’m confused here. The US has at least three major problems that Germany/Netherlands lack: nonuniversal coverage, high costs, and poor patient choice (ie you have to worry about “out of network” providers). I can see why single-payer eliminates the first: if the government buys coverage for everyone, of course it will be universal. But why does it eliminate the second two? Germany and the Netherlands have dozens of different insurance providers - why doesn’t that decrease bargaining power and raise costs? Why doesn’t it mean that sometimes they fail to reach an agreement with a hospital, and their patients can’t go there without facing “out-of-network” costs? I thought I understood the reasons why US health care doesn’t work, but Germany and the Netherlands seem to replicate its apparent disadvantages without running into the same problems. Why? Maybe I just don’t fully understand what “single-payer” means?
I’m also surprised this doesn’t get brought up more in discussions of US health reform. Medicare For All asks that we go from one of the most privatized health systems in the world to one of the most socialized, leapfrogging over successful semiprivate ones like Germany and the Netherlands. This is especially odd since those systems seem to be some of the best performers. Why would this be tempting? Absent a theory of why Germany and the Netherlands work so much better than the US, I’m not sure.
II.
Two other features of health systems caught my eye: drug price regulation and general budget setting.
No country except the US pays anything like a market price for drugs. Other countries have some Drug Price Regulator who meets and decide how much drugs will cost.
This part confused me, because it seems to be both a government decision and a negotiation. The government sets a price based on some method. Then the drug companies - well, as far as I can tell, they accept. This article makes me think that in theory drug companies have the right to refuse an unfairly low price, but that in practice neither side wants the PR hit of a country going without a drug, both sides try pretty hard for an agreement, and it’s very rare for the process to fail.
But this made it hard for me to understand this section of the book, which praised countries who managed to keep drug prices low. “Keeping drug prices low” mostly seems to involve having a process that reliably generates low numbers for the government’s offers. For example, Canada used to have high drug prices, because its process was to offer the average price paid by seven other countries: France, Germany, Italy, Sweden, Switzerland, UK, and US. But then the Canadians decided that was too high, and removed the US from their basket; since the US had the highest drug prices, this brought the average price down, and made Canadian drugs cheaper. Emanuel praises this as a good decision. But Norway does even better: they take the average of the cheapest three countries in their basket. Obviously this works, but then why not the cheapest two? Why not just say your drug price will be Norway’s price minus one dollar? Half Norway’s price? I didn’t get a good sense of why some countries had cheaper algorithms and baskets than others. Maybe they had tougher negotiators?
Also, Canada now pays the average price paid by France, Germany, Italy, Sweden, UK, and Switzerland. But Switzerland pays the average price of Austria, Belgium, Denmark, Finland, France, Germany, Sweden, UK, and Netherlands. The Netherlands pays the average price of Belgium, Germany, France, and the UK. And France says they pay the average price of “neighboring countries”. I hope someone has checked over the causal graph to make sure there aren’t any contradictions or infinite loops.
This was another place where I found myself confused about why the US system works so badly. What exactly is “market price” for a drug in the US? Consumers don’t pay for drugs directly; only insurance companies pay for drugs. In Germany, all the insurance companies get together and form a Drug Price Bargaining Group, which bargains with drug companies the same way a government would. Why don’t insurance companies do that in America? Is the problem just that this would be a monopoly (technically a monopsony, I guess?) Is only antitrust law preventing them from trying this? Is this some kind of weird horseshoe theory situation where the maximally socialist response overlaps with the maximally libertarian one?
If you think drug price bargaining feels more like magic than economics, you’ll love the concept of health care budget setting. The idea is: the country decides how fast it wants health care costs to grow in a certain year, for example, “prices must not rise more than 1% this year”. Then they calculate it out and find that a 1% rise in prices corresponds to a health care budget of $1 billion or whatever. Then doctors submit reports on how much health care they’ve done, ie “we have done 500,000 units of health care”, according to some list where a blood test counts as X units, a heart surgery as Y units, etc. Then the government says “Well, we said the budget was going to be $1 billion, doctors did 500,000 units of health care, so we’ll reimburse doctors $2,000 for each unit of health care they did”. If instead doctors say they’ve done 1,000,000 units of health care, the government will only pay them $1,000 per unit. And so on.
I spent a long time staring at this system trying to figure out how it could possibly work. I think if the government will pay you $2,000 per unit in 2020 and only $1,000 per unit in 2021, then you stop doing all the health care with a value of between $1,000 and $2,000 per unit, which reduces this to the usual “if you pay less money, you get less stuff” situation. If costs rise faster than the budget, your care gets worse every year, but in real life this doesn’t seem to happen. No, I don’t know why not.
Overall I got the impression that health care was a bizarro-world where normal economics doesn’t apply. If you have the courage to say loudly and firmly “we refuse to pay a high price for this”, then providers have to give you a low price, and your health care system will be great and affordable. Seems hard to believe, but the US sure does pay twice as much per capita as countries that go with the “loudly refuse to pay more than a certain amount” strategy. I would have appreciated a book by a more economically-minded person explaining why things are like this. Or maybe not; maybe it’s like quantum physics, and the second someone looks at it too closely, the whole structure will collapse, every hospital in the world will go bankrupt, and we’ll have to get our medical problems treated by wolves.
III.
Emanuel deserves a lot of praise for writing this book. It’s hard to find good information on different health care systems outside of incomprehensible technical papers. This book was detailed, thorough, and got me to start investigating a field I’d been putting off learning about.
But it failed to give me a gears-level understanding of why some health care systems succeed and others fail. In fact, the main knowledge it gave me was negative: I realized that my pre-existing ideas of why US healthcare is so bad didn’t really make sense, since other countries do similar things with better results.
It didn’t make me feel like I understood the tradeoffs of health economics. Why do some countries set lower prices for drugs than others? What good or. bad things happen if you deliver single-payer care through the government vs. through nonprofit insurance funds? How does the US model (which doesn’t work) differ from the superficially-similar Swiss, German, and Dutch models (which do)?
The main thing I would have done differently was change the division of chapters. Emanuel had one chapter on each health care system, with subchapters on how it handled hospitals, how it handled drug prices, etc. But it was hard to remember what the last system had been like, and many systems were similar enough that it felt like reading the same bureaucratic structure over and over again. It might have been more readable if there had been a chapter on (eg) hospitals highlighting the different ways hospitals could be run, which countries chose which methods, and which ones seemed to work best. Then another chapter on drug prices, and so on.
I was also sad at the limited selection of 11 health care systems this book presented. I could have done with much less detail on the exact three-letter-acronyms used by Germany vs. France, and more exploration of genuinely novel systems. What do developing countries do? What about the former Soviet states? What about the way the USA worked in 1950, or 1900, or still works today if you’re Amish? These probably aren’t the World’s Best Health System, but they would at least help me understand the dimensions along which systems can vary.
In conclusion, this was a helpful book. But I’m not sure it’s worth paying $22.99 for it. Consider telling Dr. Emanuel that you will only pay however much the Norwegians pay for their books. Or maybe the lowest price paid by any of Belgium, France, or Germany. Maybe you should commit to only spending $100 on books this year, and let Dr. Emanuel know how much you’ll pay him after you decide how many books to read. Only then will we be able to control the spiraling cost of books on health care.
 .
.