Diseasonality
[epistemic status: conjecture and speculation in something that isn’t really my field]
I.
It’s still not totally clear why some diseases are seasonal.
Seasonal diseases usually peak in late winter - so around January/February in the Northern Hemisphere and July/August in the Southern. Around the equator, which lacks seasons, they’re less predictable and happen throughout the year. The best known seasonal diseases are flu and colds. But viral diarrhea and chickenpox also qualify, as do older mostly-eradicated diseases like measles and diphtheria.
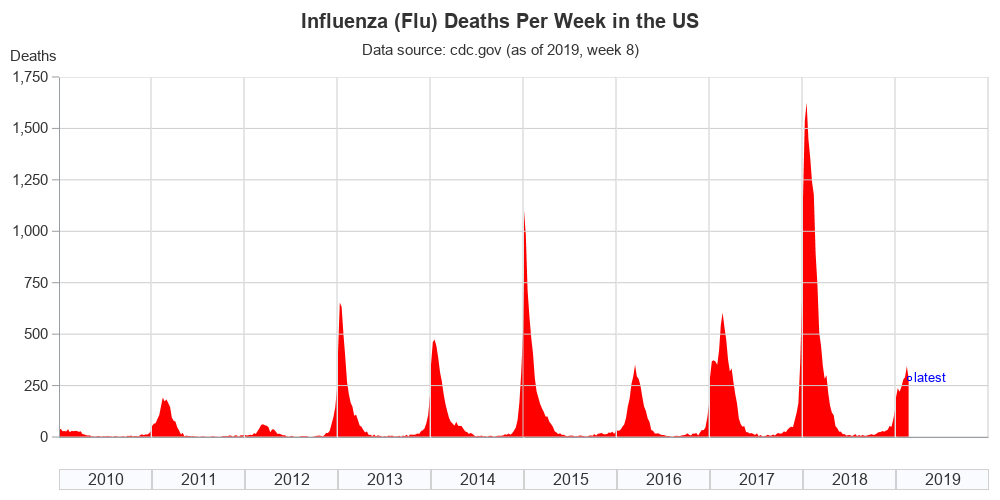 The seasonal flu (source)
The seasonal flu (source)
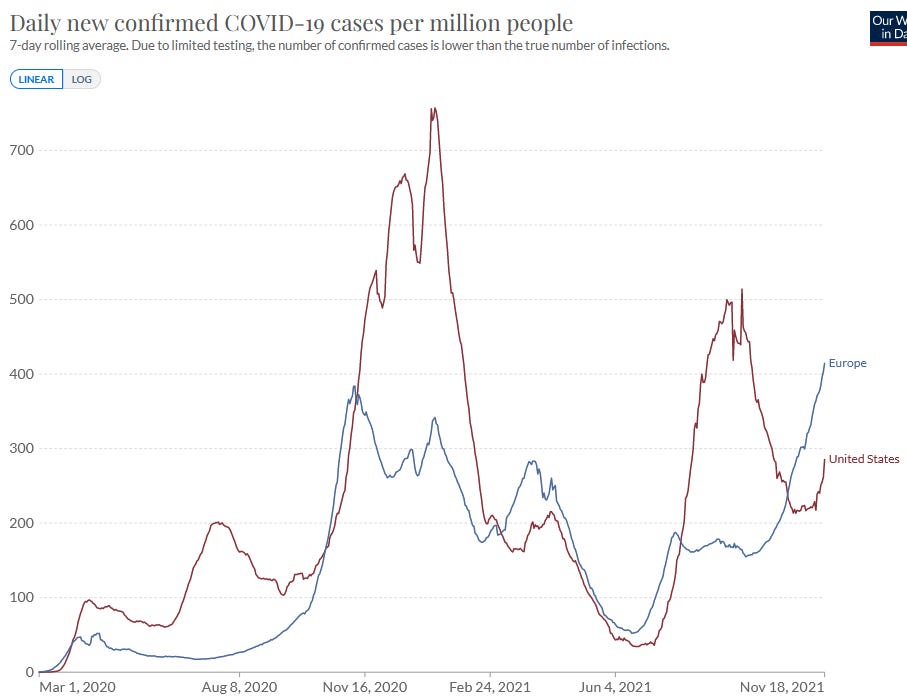
The novel coronavirus is probably seasonal-ish, although it’s hard to tell since so much stuff keeps happening to make it better (vaccines) or worse (new variants).
The most common theories for disease seasonality are:
-
Pathogens like the cold
-
Pathogens like low humidity
-
People are cramped indoors during the winter
-
People have low vitamin D during the winter, and vitamin D helps fight pathogens
None of these are really satisfactory on their own.
Cold and humidity are definitely important - scientists can make flu spread faster or slower in guinea pigs just by altering the temperature and humidity of their cages. But it can’t just be cold and humidity. But if it was just cold, you would expect flu to track temperature instead of seasonality. Alaska is colder in the summer than Florida in the winter, so you might expect more summer flu in Alaska than winter flu in Florida. But Alaska and Florida both have lots of flu in the winter and little flu in the summer.
(if it was just humidity, same argument, but change the place names to Arizona and Florida.)
It’s the same story with people being cramped indoors. Common-sensically, this has to be some of the story. But if it were the most important contributor, you would expect to see the opposite pattern in very hot areas, where nobody will go out during the summer but it’s pleasant and balmy in the winter. Yet I have never heard anyone claim that any winter diseases happen in summer in Arizona or Saudi Arabia or terrible places like that.
If it was just vitamin D…look, it’s not vitamin D. Nothing is ever vitamin D. People try so hard to attribute everything to vitamin D, and it never works. The most recent studies show it doesn’t prevent colds or flu, and I think the best available evidence shows it doesn’t prevent coronavirus either. African-Americans, who are all horrendously Vitamin D deficient, don’t get colds at a higher rate than other groups (they do get flu more, but they’re vaccinated less, so whatever).
Might it be some combination of these things? Maybe Alaska is cold all year, but gets drier in the winter? Maybe people stay indoors in Arizona in the summer, but it’s not cold enough for flu to spread? If you came up with some multidimensional dryness-coolness-indoorness metric, then maybe places could be high on one or two in the summer, but the combined metric would always be highest in the winter everywhere.
This is possible. I just find it hard to believe that the place where this metric is highest in summer doesn’t even overlap with the place where the metric is lowest in winter.
II.
What about ultraviolet light?
This has been getting more press recently as people realize that UV kills pathogens and that this might be part of the reason outside seems safer than indoors.
Does this fail by the same argument as cold and humidity? That is, does Florida in winter get more ultraviolet light than Alaska in summer? Here’s what a paper has to say:

It’s a bit weird! In summer, polar and tropical areas get about the same amount of UV; in winter, the tropical areas stay about the same and the polar areas crash to almost zero.
See also the world’s most annoying and hard-to-read graph, from Nicastro et al:
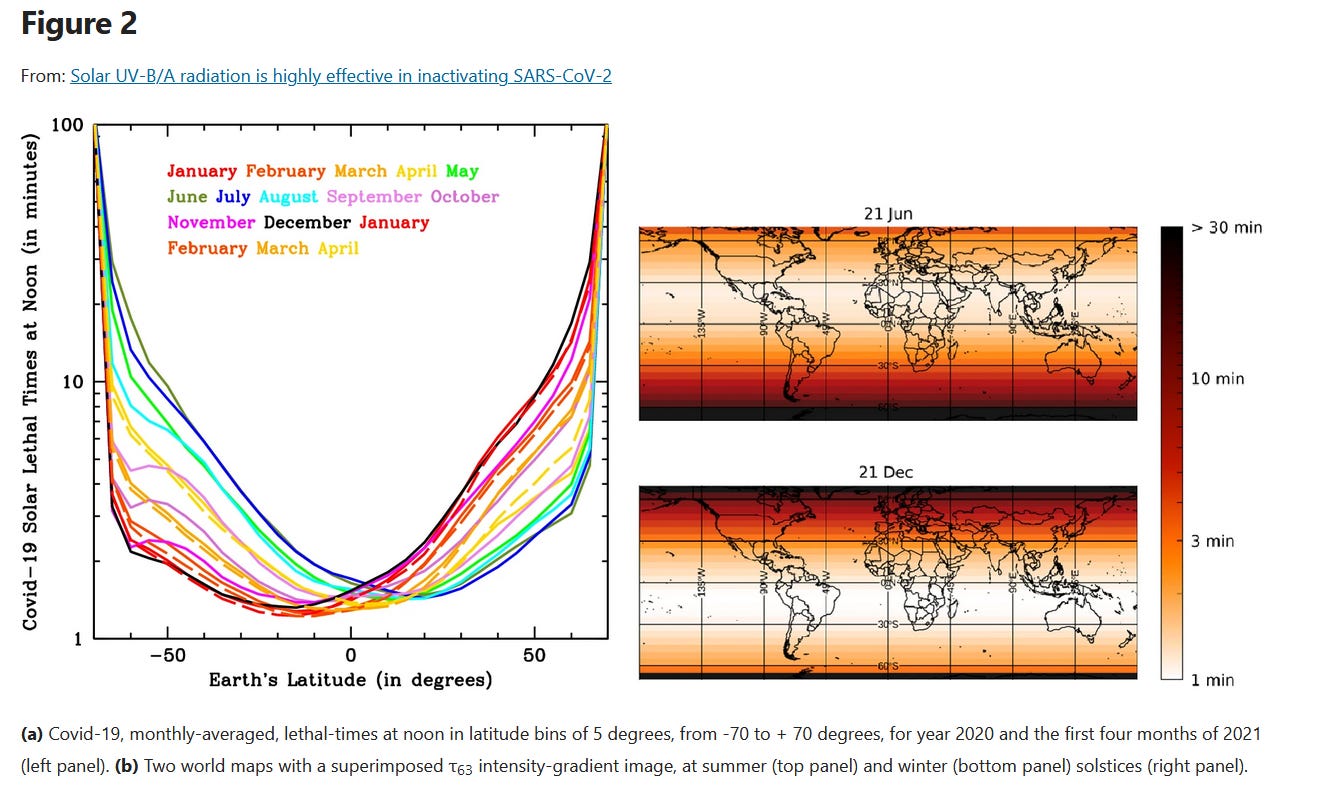
Look at the left figure, and focus on the dark blue line (July) and dark black line (December). Miami, Florida, is at a latitude of 25 degrees; Juneau, Alaska, is at about 60. If I’m reading the graph right, Miami in December gets enough UV to kill a virus in two minutes. Juneau in July gets enough UV to kill a virus in…also about two minutes.
How much can UV matter? After all, most people are inside in the winter anyway. One possible answer is that it doesn’t matter much in these situations, but it’s a good explanation for why eg Arizona (where people are inside in the summer) still gets a seasonal flu in the winter. Another possible answer is that as far as I can tell even indoor UV light can matter. About 75% of UV-A radiation gets through window glass. Although most people think of UV-C or even UV-B as the most effective antiviral agent, another annoying and hard-to-read graph from Nicastro et al suggests otherwise:
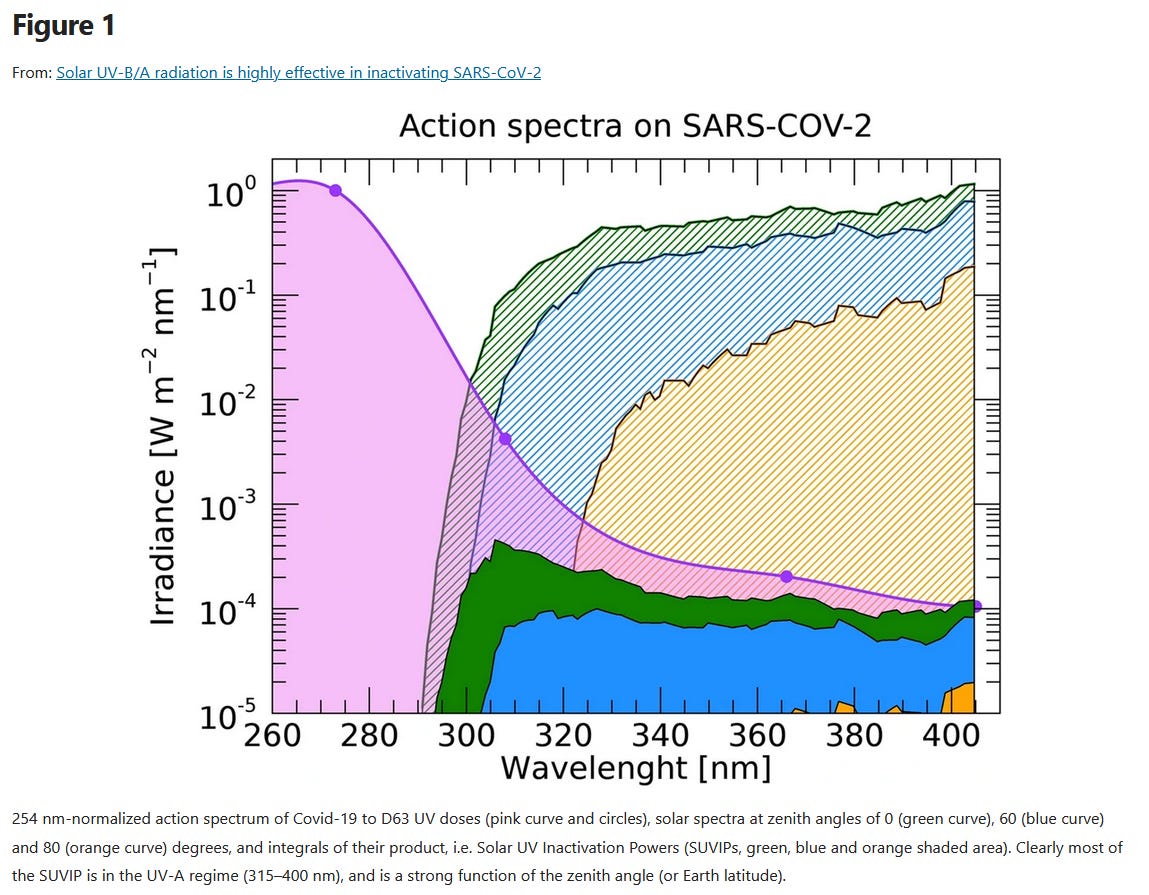
This doesn’t mean 75% of UV’s viral killing power makes it inside - unless you live in a greenhouse, only a tiny bit of your house is windows, so no matter how much light each window lets through most of the sunlight will get blocked. I’m not really sure how to model this because it might depend on a virus particle’s chance of getting hit by a sunbeam, which depends on a lot of factors. Still, it doesn’t seem impossible to me that ambient UV levels can matter even indoors.
The same amount of UV light reaches Alaska in the summer as Florida in the winter. But that means that even if UV was the entire explanation, we could only explain why Alaskan summer is no worse than Floridan winter in terms of flu. But Alaskan summer isn’t just no worse than Floridian winter, it’s actually much better.
So we can add UV to our combined multi-dimensional metric idea, and it will improve it a little. But I’m still not completely satisfied with it. Seasonality seems too strong, even after you account for all these factors.
III.
What happens when we think about this dynamically?
Suppose that Arizona, uniquely among places in the world, is more vulnerable to flu in summer than winter. But if all Arizona’s neighbors are flu-free in summer but severely-impacted in winter, they would be more likely to transmit the flu to Arizonans in the winter. Or if all new flu strains originate in China, and China develops a new flu strain in the late autumn, then it will sweep across the immunologically-naive world in winter, and Arizona will get hit just like everywhere else.
On a first pass, this doesn’t really work. The coronavirus seemed seasonal last year, but it was already everywhere, and there were no new strains (last winter was before the variants mattered much). Also, consider Australia. It’s in the Southern Hemisphere, so its winter is northern hemisphere summer. But it gets its flu season during its own winter, not ours. It doesn’t follow China’s timeline, and it doesn’t follow the timeline of travelers who might be bringing in flu cases (I assume most of its inbound travelers come from the Northern Hemisphere).
But on closer inspection, something like this seems to be going on in some places. This article looks at flu in the northern tropical parts of Australia in particular. Big southern Australian cities get flu seasons in their winter (ie July). The tropical parts of Australia are near the equator and don’t naturally have seasons, but they usually get a flu season in July anyway. But occasionally they’ll get a flu season in December, or even both in the same year! Most likely what’s happening is that they have no natural flu season, but people have to get the flu sometime, and they usually get it when travelers from the rest of Australia bring their flu cases in, but sometimes they also get it when travelers from the Northern Hemisphere bring their flu cases in.
The part I find interesting here is that flu spikes are more fundamental than flu seasonality. Deprived of seasons, a place doesn’t just have a slow burn of flu cases all year. It has a big epidemic, then dies down for a while, then has another big epidemic. In retrospect, this is an obvious consequence of how diseases work (eg the SIR model of transmission). Some people get the disease, it spreads exponentially until lots of people are immune, and then it stops until something changes.
And it happens once or twice a year. Why? Maybe a new variety comes out of China every year, but that doesn’t explain the occasional twice-yearly spikes in tropical Australia. The article I find most enlightening here is this New York Times piece from summer 2021: Why Everyone Has The Worst Summer Cold Ever. It says that lots of people got bad colds (particularly colds spread by a pathogen called Respiratory Syncitial Virus) in summer 2021, after coronavirus restrictions were loosened. RSV is usually very seasonal and very winter, so presumably there was “built-up” RSV vulnerability that got a chance to break out once COVID restrictions were loosened. The article even says:
Although your immune system is likely as strong as it always was, if it hasn’t been alerted to a microbial intruder in a while, it may take a bit longer to get revved up when challenged by a pathogen again, experts say. And while some viral exposures in our past have conferred lasting immunity, other illnesses may have given us only transient immunity that waned as we were isolating at home.
“Frequent exposure to various pathogens primes or jazzes up the immune system to be ready to respond to that pathogen,” said Dr. Paul Skolnik, an immunovirologist and chair of internal medicine at the Virginia Tech Carilion School of Medicine. “If you’ve not had those exposures, your immune system may be a little slower to respond or doesn’t respond as fully, leading to greater susceptibility to some respiratory infections and sometimes longer or more protracted symptoms.”
[…]
“I haven’t seen anything like this in 20 years of working as a virologist,” said Dr. Huang. “There’s usually a degree of pre-existing immunity due to the previous winter. When you don’t have that kind of protection, it’s a bit like a wildfire. The fire can just continue, and the chain of transmission keeps going.”
I think maybe they’re saying something like that getting a virus like this usually gives you about a year’s worth of immunity before your immune system “forgets” it. I guess this makes sense in the context of eg needing COVID “booster shots” after a few months.
So one possible model is something like: once you get a disease, you’re protected for a while. There’s no particular length of time, it’s a spectrum, absent any external rhythm-setter you would end up like the tropics, where people have epidemics at random times, once a year, twice a year, whatever.
But the seasonal cycle “entrains” this rhythm (cf. the idea of a zeitgeber). It offers a good way for everyone’s inconsistently-and-gradually-declining immunity to get below the threshold where an epidemic can start at the same time.
So in the tropics, Florida, and Alaska, epidemics “want” to follow a cycle of coming approximately once a year. In the tropics, nothing is giving them that cycle, so they come at a random time once a year, or twice a year, or whatever. In Florida, UV light, temperature, etc provide that cycle, and they come once a year. In Alaska, UV light, temperature, etc also provide that cycle, and they come once a year independent of what’s going on in Florida. It’s like the saying about how you don’t have to outrun the bear, you just have to outrun the other hikers. July in Alaska doesn’t have to outrun January in Florida, it just has to outrun January in Alaska, for the dubious honor of when Alaska’s destined-to-be-once-a-year flu season is going to be.
IV.
Right now I think the coronavirus is about halfway to being a seasonal disease.
Judging by the speed at which people need booster shots for their vaccines, the coronavirus probably has non-permanent immunity (this is far from proven - vaccines could work differently from whole viruses - but it seems plausible). If its period is anywhere close to a year, the seasonal cycle of temperature/UV/etc will probably entrain it to a once-a-year rhythm.
But right now it’s not in that rhythm, because there are still lots of people who have never had it at all. So absent any other factors (lockdowns, vaccines, new variants, etc) what we might expect to see is something like coronavirus spreading through the population at some steady rate in the summer, and then some faster steady rate during the winter when conditions are more favorable. Eventually it would infect everyone, and then we would expect to see it barely at all during the summer, followed by a spike in the winter.
Right now there are lots of other factors, but we still sort of see that pattern. Nicastro et al continue their perfect record of annoying hard-to-read graphs:
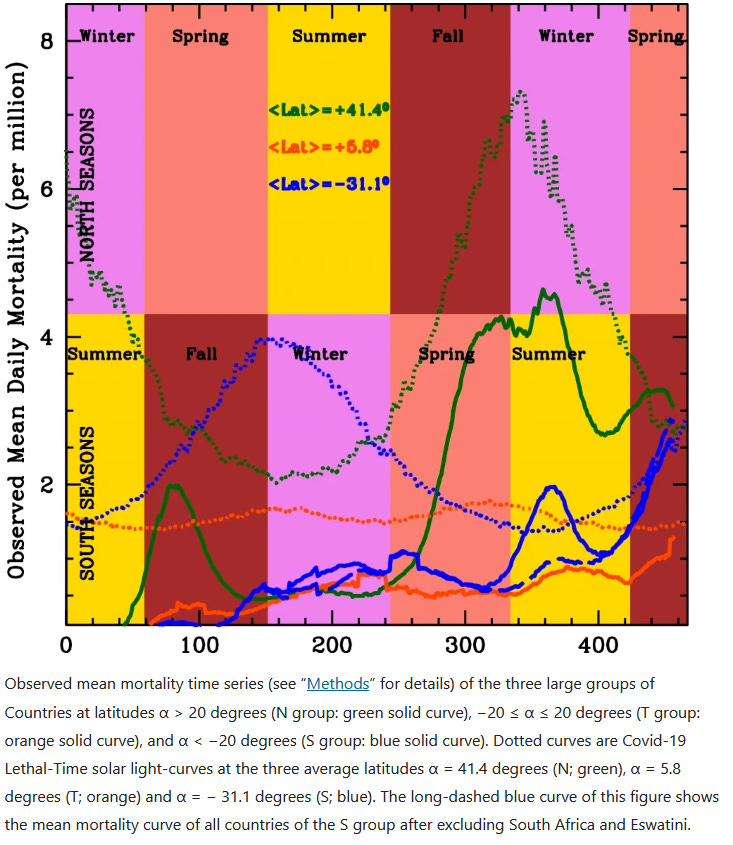
The solid green line is COVID cases in the northern hemisphere, the solid orange line is COVID cases in the tropics, and the solid blue line is COVID cases in the southern hemisphere. The top set of technicolor background squares shows northern hemisphere seasons. So we see that COVID in the northern hemisphere peaked twice - once when it first started existing, and once in northern hemisphere fall/winter. COVID in the southern hemisphere shows a less obvious pattern, with maybe a mild peak in southern hemisphere fall winter, disguised by other factors. It peaks again around day 350 in a way that is very awkward for this theory, but the researchers say this is just because the Beta variant was ravaging South Africa at that time - the long-dashes blue line shows what happens if you adjust that away, at which point the southern hemisphere mortality pattern looks seasonal again. Meanwhile, the tropics are just sort of hanging out, not showing any pattern at all.
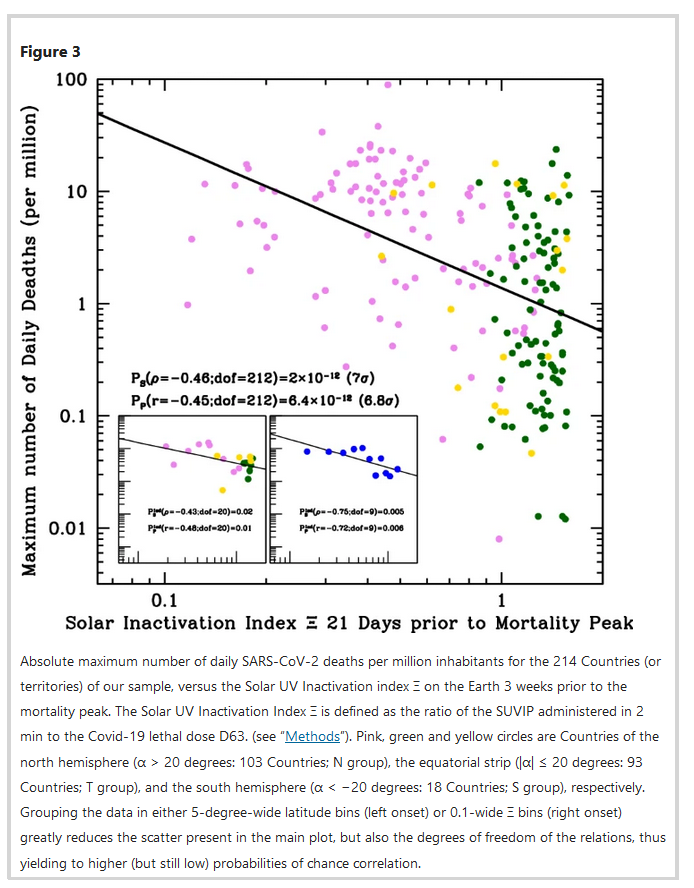 The more formal version of this.”Simple linear-regression tests of the data-points (Pearson) and their rankings (Spearman), yield null (i.e. chance correlation) probabilities of p = 6.4 × 10–12 and p = 2.0 × 10–12, respectively.”
The more formal version of this.”Simple linear-regression tests of the data-points (Pearson) and their rankings (Spearman), yield null (i.e. chance correlation) probabilities of p = 6.4 × 10–12 and p = 2.0 × 10–12, respectively.”
So possibly coronavirus is still in its half-seasonal phase, and will transition to a fully seasonal disease once it’s infected everyone it can infect and picked all the low-hanging fruit in possible-variant-space so that it can’t trivially become more infectious.
Can we use our improved understanding of disease seasonality against it? Certainly these considerations suggest that doing various things to indoor air (and using indoor UV lights) could slow transmission. But this wouldn’t lead to an eternal summer of perfect viruslessness. At best, it would just put us in the same position as the tropics, where there’s nothing to constrain the disease’s rhythm, and it just strikes randomly.