Highlights From The Comments On Geography Of Madness
[Original post:The Geography Of Madness]
Thomas Reilly (author ofRational Psychiatry) writes:
I don’t think Bouffée délirante is a culture bound syndrome - it’s just the French equivalent of brief psychotic disorder (DSM), acute and transient psychotic disorder (ICD), or Brief Limited Intermittent Psychotic symptoms (CAARMS). [See] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8581951/
I responded “Have you ever seen BPS? I almost never have, and was told it was mostly used as a code for new-onset schizophrenia that didn’t satisfy the time criterion yet,” and Dr. Reilly wrote:
Yes, in the context of an At Risk Mental State service, where it makes up roughly 20% of referrals https://www.sciencedirect.com/science/article/pii/S0924977X20302510 .
This is a really good point, and I appreciate his prodding on this matter. I’m trying to remember how often I’ve a boufee delirante/ brief psychotic syndrome-like cases, and realizing how hard a question this is. I’ve definitely seen people suddenly become psychotic for no reason, but I usually assume it’s because of drugs. I can’t always establish this right away, because the person might be too psychotic to answer questions, but usually in the end when I’m able to get the full story the assumption about drugs proves true. Does it always? I don’t think my mind keeps track of that statistic, which means that cases of BD could easily slip through my radar.
Related: the DSM doesn’t let you diagnose schizophrenia until someone’s been having symptoms for six months. What happens if you see someone one month into what seems likely to be schizophrenia? You provisionally diagnose Brief Psychotic Disorder until the six month mark. But newly psychotic people are often randomly getting better or worse from day to day, and getting shuffled from ERs to inpatient wards to partial programs to at risk programs, and in all of this shuffling it would be hard for an individual psychiatrist to notice someone who actually was just psychotic for one month and then recovered and was completely normal.
Given how complicated it is to notice this diagnosis, I now wonder whether the differences between France (where doctors have a low bar for noticing and diagnosing this) and everywhere else (where they have a high bar) require explanation.
Steve Sailerwrites:
The first Columbine-style school shooting I am aware of was at the U. of Texas around 1966. The next was a young woman shooting up a school outside of San Diego around 1978. When asked why she did it, she said, “I don’t like Mondays.” Bob Geldof of the Boomtown Rats wrote a catchy tune about that shooting, which likely helped make school shootings more of a Thing in American culture.
In contrast, some things that used to be bigger Things in America seem to have receded somewhat, such as serial killings, political assassinations, bombings, kidnappings, and skyjackings.
This encouraged me to look into the school shooting statistics further, and I take back my claim that Columbine was a break from trend. This article claims the first mass shooting in US history was in 1949, and that the initiating factor seemed to be advances in gun technology; there have been violent sprees since forever, but semi-automatic weapons raised the death count to levels that made national news.
If this is true, I’m not sure what survives of amok as a specifically Malaysian culture-bound illness. Perhaps the victim’s claim to be possessed or amnesiac is uniquely Malay, but surely if Americans could get away with saying a tiger spirit made them do it, they would try that too!
In fact, this would be a good place to admit I’m getting very skeptical about pretty much every culture-bound syndrome on the traditional list. Amok and boufee deliriante impress much much less after reading your comments, and the other big famous one is taijin kyofusho, a supposedly a Japanese culture-bound condition where someone is excessively . . . I’m trying not to use the words “socially anxious” so that it can be a big reveal when I say it seems similar to our Social Anxiety Disorder.
The culture-bound aspect is supposed to be that it presents differently, with fear of causing offense. But first, many Americans with social anxiety disorder fear causing offense. And second, everyone knows that Japanese culture is more offense-focused than ours; “Americans and Japanese express social anxiety in different ways” feels less mysterious than “they have completely different culture-bound mental disorders!”
Another thing going on seems to be a problem of grouping: one sub-aspect of taijin kyofusho is shubo-kyofu , basically body dysmorphic disorder. American psychiatrists would never think of this as a kind of social anxiety, but it kind of fits. Another symptom is jikoshu-kyofu , fear of body odor. I’d never heard of this and thought it might be a genuine Japanese culture-bound condition, but Wikipedia tells me there’s a Western version called olfactory reference syndrome. The International OCD Foundation says that “the prevalence of ORS is not known, but it is certainly more common than generally recognized”. Lochner and Stein find that the prevalence in psychiatric samples (ie people with other mental health conditions) seems to be around 2%. I don’t think it’s at all obvious that more Japanese than non-Japanese have this condition that nobody ever does a good job measuring the prevalence of.
The other culture-bound illness I mentioned on the post was shenkui , a Chinese condition where people who believe in yin and yang feel like orgasming depletes them of vitality. But isn’t this pretty similar to r/NoFap? I imagine that before there was Reddit, there were a lot of Westerners individually thinking “I feel worse and sicker every time I masturbate”, but never mentioning it because nobody wants to hear about your masturbation habits.
All of this is convincing me that culture bound illness, while real, is much subtler than The Geography of Madness (or my previous views) suggested. Or maybe that the panic type (where they spread in epidemics over the course of a few days) are more culture-bound, but that the long-run normal conditions are less culture-bound than I thought.
Morganwrites:
This paper found widespread PTSD symptoms among warriors in a pastoral African society, suggesting that it’s not culture-bound. .
From the abstract:
“It is unclear whether combat-related PTSD is a universal evolutionary response to danger or a culture-specific syndrome of industrialized societies. We interviewed 218 Turkana pastoralist warriors in Kenya, who engage in lethal cattle raids, about their combat experiences and PTSD symptoms. Turkana in our sample had a high prevalence of PTSD symptoms, but Turkana with high symptom severity had lower prevalence of depression-like symptoms than American service members with high symptom severity. Symptoms that facilitate responding to danger were better predicted by combat exposure, whereas depressive symptoms were better predicted by exposure to combat-related moral violations. The findings suggest that some PTSD symptoms stem from an evolved response to danger, while depressive PTSD symptoms may be caused by culturally specific moral norm violations.”
Great find! This study looks at the Turkana people of Kenya. Even though they are a very warlike society (“half of adult male mortality stemm[ed] from combat”), the authors find that many of them had PTSD (they draw a distinction between “learning and reacting symptoms”, which were equally common among Turkana and Americans, and “depressive symptoms”, which were less common in Turkana, but it didn’t seem like a huge effect.) There are a few sentences suggesting they limited their analysis to the Turkana who seemed to have a lot of PTSD, which would be relevant, but they didn’t have much trouble finding them.
McChemistwrites:
My wife was a teenager growing up in Hong Kong in 1994, and she says she (and presumably her classmates) had known what anorexia was before this schoolgirl died. She posits that the ensuing rush of cases was a function of diagnosing an existing disease, not of a cultural idea getting implanted. Single data point and all that, make of it what you will.
Thanks for this. I’m realizing I have only Ethan Watters’ account of how unknown anorexia was in pre-1994 Hong Kong, and that this is exactly the kind of exciting cultural difference that often people play up and then have to ashamedly back down from later when more dedicated anthropologists show up on the scene.
AntiMemeticsDivisionDirectorwrites:
I remember when I was in middle school there was a big awareness campaign around cutting. Assemblies, guest speakers, special sessions of health class, material sent home to parents, etc. Immediately, the number of (predominantly) young women cutting went way up - or at least the number cutting in highly visible locations did. The next year things were mostly back to “normal”. Of course there’s no way to know for sure, it’s entirely possible that those people prominently displaying scars would have been self harming in some other way without the campaign, but it was striking to 7th grade me.
Don’t misunderstand me, I don’t mean to imply that cutting didn’t exist before or stopped existing afterward. And I’ll grant that middle schoolers may not be the most representative population. But from an early age I observed that
a. While mental illness has always existed, the specific ways in which it manifests can be extremely malleable, and
b. When you make it clear to people - especially awkward, insecure young people - that compulsive behavior X will result in receiving large amounts of sympathy and positive attention, expect rates of compulsive behavior X to go up. To be clear that doesn’t necessarily mean people are faking behavior X (although in hindsight I suspect some of those scars were drawn on), but when social incentives are powerful and sudden people will alter their behavior in surprisingly radical ways.
…and that’s why they became the antimemetics division director!
Seriously, there was a very similar episode in The Geography Of Madness. A Chinese school was having a few cases of koro, and:
Two days later, on May 23, when the school principal learned about the incident, he gathered all the students (393 boys and 287 girls, 680 in total) together in the school courtyard. Using a microphone, the principal explained to the students in detail what had happened, and warned them to be cautious, and to take emergency measures if they experienced similar symptoms.
That day, several boys felt their penises shrinking and rushed home to get treatment. The following day, sixty more students were struck with suo yang.
Teucerwrites:
I think you’ve got the etiology of the rise in trans identities more or less backwards, but your note that there is no neutral culture rescues you from actually saying anything false. I think we’re not so much seeing a result of a stronger cultural sense of being the wrong gender (that probably peaked in the 80s), as we are a weakening of our culture’s ability to assign gender at all.
Sex is biologically real. Intersex people are a small, but not statistically negligible, fraction of the population, and the rest of us do fall into two categories with regard to our outward sexual characteristics. But what traits do those sexual characteristics assign?
In 21st-century America, women are less enthusiastic about sex, often unsatisfied by it; therefore, it’s only natural that men initiate most sexual encounters. In ancient Athens, women, the irrational sex, were slaves to their desires, and part of the humor of the Lysistrata was the idea that the women took their protest so seriously that they could restrain their sexual appetites.
In 21st-century America, mentioning that a man writes whiny poetry is a great way to call his masculinity into question. In 12th-century England, Richard the Lionheart was the epitome of manliness, and was especially praised for being a warrior poet. Only one of his poems survives (Ja Nus Hons Pris) and it’s pretty whiny.
Anthropologists who study gender find gender categories like that in every culture, with anywhere from two to five genders. America right now has two, but its ability to assign those two is breaking down.
Weak prediction (call it 40%, with a very low chance that our current systems hold and a decent chance of something I don’t foresee happening instead): in 2073, American culture will have three gender categories that are pretty well respected, with most trans people born after 2048 being in the middle gender (currently called “non-binary”, which isn’t just one thing now but is seen as one thing then) rather than being AFAB trans men or AMAB trans women. 20%: any attempt to explain what it is to be male in 2073 seems kinda nonsensical; 90%: any such attempt remains very controversial.
(Disclosure of biases: I’m a cis man that’s also comfortable with neutral pronouns.)
I agree with the first paragraph; I think saying “more people are being socialized into transgender” and “fewer people are being socialized into cisgender” are more or less identical. David Chapman writes about the “choiceless” nature of traditional societies; if you were born in a peasant village in medieval England, you would be straight, cis, Christian, monarchist, and a farmer - neither because you loved those things and chose them voluntarily, nor because evil outsiders forced you to do those things which you secretly hated, but because you couldn’t conceive of doing anything else. Very gradually, that choiceless mode broke down into the package of identity choices people face today; faced with the choice between being cis and trans, some people find that something (maybe biology) gives them an extremely strong pressure towards trans; if they didn’t realize that was a choice, the pressure might come out some other way, or just fizzle out.
Maybe this is an argument for gender dysphoria not being like culture-bound mental illness; I don’t think there’s any sense in which, given a choice to believe that a witch stole your penis, some people are going to choose yes.
Regarding PMS and PMDD, Aella writes:
I read this book a while back and got curious about PMS. Here’s a twitter poll that showed a decent correlation between believing in ghosts, and getting PMS:
(source)
(tho I’m slightly more wary of twitter polls that I can’t include ‘see results’ options in)
I then also added in a question about PMS to my big kink survey, asked to biological females only. I’m in transit (and my dataset got too huge so can’t rerun it until I figure out how to run it from a hosting service) rn but can share any correlations with that soon.
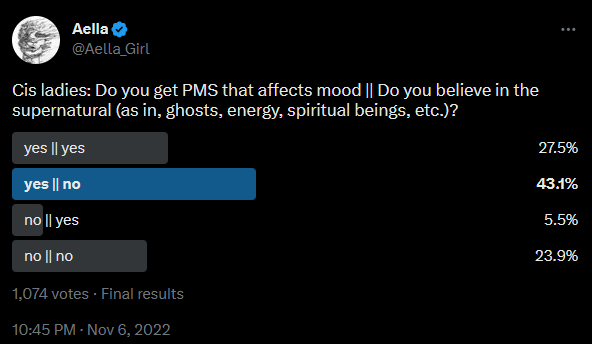
If I’m reading that poll right, many more ghost believers than ghost skeptics get PMS. I am boggled by this and Aella is a national treasure - although I look forward to her reporting the more formal investigation of this in her survey.
I don’t think it’s obvious that “believes in ghosts” is a proxy for “more likely to develop culture-bound illnesses”, but I can’t think of a better reason why these should be so connected.
Aella also has written about her own experience with trauma - and how it changed once she left her culty upbringing, learned what trauma was, and understood that other people expected her to have it - here.
Analytic Converterwrites:
In my freshman year of college, my roommate, who was a violin major, got crippling tendonitis in her forearm, presumably from suddenly playing the violin vastly more hours of the day. (Eventually she changed majors.) Guess who ALSO got crippling forearm tendonitis, despite no corresponding lifestyle change? Me. I’m like 99% sure this was social contagion, but the tendonitis was real.
There is a contingent of people who think of tendonitis, repetitive stress injury, carpal tunnel, etc as somewhere between 50% and 99% cultural. I think it’s probably a mix, but I’ve been told some people with carpal tunnel have benefitted from Unlearn Your Pain and similar books, and I weakly recommend them to such people, as an experiment.
Markwrites:
About the ol-german poem “by” Hans Vitler ‘flowers of virtue” - that was a translation of an Italian original form 1320* Hans Vitler’s famous translation was rather “free”, but I guess he would not have added a penis-theft. - Now I found one commented reprint of “Blumen der Tugend” , well actually “Pluemen der Tugent” - it is oooold: https://archive.org/details/diepluemendertu00maxigoog/page/n381/mode/1up no such story there, it seems Vitler considered believe in witchcraft even: sinful superstition. Witch-hunt was NOT a middle-age thing, but came big in (early) modern times. Prof. Marvin Harris has some theories as for “why then”: Cows, Pigs, Wars, and Witches: The Riddles of Culture (tl;dr: both big churches THEN felt the need to proof they were “indispensable” - before: the one church just obviously was. Witch-hunts: ON.)
- seems one can find here - it translated automatically(?) on my chrome at least (into a strange kind of modern German) : https://it.wikisource.org/wiki/Fiore_di_virt%C3%B9/I
tl;dr: speed reading it; i saw no witch or penis-theft, though the beginning of the text starts rather misogynistic
Weird. My source said it came from Flowers of Virtue, 1486, but Flowers was published earlier than that, and Malleus was published in 1486, so maybe it’s confusing these and this is a Malleus illustration?
Garaldwrites:
I’m surprised that nobody has mentioned an obvious contributor to that-witch-stole-my-penis: testicles do retract, and penises do shrink, as an unconscious response to fear! Not all the way into the body cavity, obviously, but they do retract and shrink to a very clear effect. (It’s a reflex that is probably there to, well, safeguard our balls.) You can see how this works now: if you get really afraid of an imaginary penis-stealing witch in the neighborhood, your bits will noticeably retract, thereby confirming your fear of the penis-stealing witch. The very real sensations you perceive as a result of the cremaster actually doing its work will be amplified and interpreted by your witch-believer brain in the way you’d expect.
This is a good point. I had kind of discounted it, because many koro patients say their penis is missing, not just smaller or retracted, and I find it hard to imagine my penis retracting so far that I start believing it’s not there. Maybe I just haven’t been sufficiently afraid. Somebody should watch a horror movie naked, then report back. For science.