Highlights From The Comments On Ivermectin
Thanks to everyone who commented on my recent post Ivermectin: Much More Than You Wanted To Know.
Let’s start with the negative comments. Leading pro-ivermectin website ivmmeta.com understandably disagreed with my fisking of them. They have a section where they respond to critics (see responses to Gideon Meyerowitz-Katz, to the BBC, to the parasitic worm hypothesis, and to someone named AT who they won’t explain further). I was honored to also get a response here. They write:
We note a few limitations and apparent biases in the SA/SSC ivermectin analysis.
Author appears to be against all treatments, labeling them all “unorthodox” and “controversial” , even those approved by western health authorities, including casirivimab/imdevimab, bamlanivimab, sotrovimab, and paxlovid.
We encourage the author to at least direct readers to government approved treatments, for which there are several in the author’s country, and many more in other countries (including ivermectin). While approved treatments in a specific country may not be as effective (or as inexpensive) as current evidence-based protocols combining multiple treatments, they are better than dismissing everything as “unorthodox”. Elimination of COVID-19 is a race against viral evolution. No treatment, vaccine, or intervention is 100% available and effective for all variants — we need to embrace all safe and effective means.
Author notes that: “if you say anything in favor of ivermectin you will be cast out of civilization and thrown into the circle of social hell reserved for Klan members and 1/6 insurrectionists” , suggesting an environment that may bias the information that the author sees, and could unconsciously bias analysis. We note that similar environments influence the design, operation, and publication of some existing (and many upcoming) ivermectin trials.
Author briefly looks at 30 of the 66 studies, which we note is much better than most commenters, but still ignores the majority of studies, including the prophylaxis studies.
The author finds efficacy at p = 0.04 in their analysis of 11 of the 30 studies they looked at. We note that simply looking at the other 36 studies will result in much higher confidence in efficacy. We also note that even at p = 0.04 with 11 independent studies, a rational risk-benefit analysis results in immediate adoption into protocols (pending stronger data with other combinations of treatments), and immediate collection of more data from sources without conflicts of interest.
However, ultimately the author at least partially supports the two prevailing theories that are commonly used by those against treatment. These theories require disregarding extensive contradictory evidence:
The steps required to accept the no-significant-effect outcome are extreme — one needs to find a reason to exclude most of the studies, disregard the strong treatment-delay response relationship, and disregard all prophylaxis studies. Even after this, the result is still positive, just not statistically signficant. This does not support a negative recommendation. Widely accepted and effective (subject to dependence on viral variants) treatments like casirivimab/imdevimab, bamlanivimab, and sotrovimab were all approved without statistically significant mortality benefits.
The steps required to accept the strongyloides-mechanism-only conclusion are also extreme - we need to disregard the majority of outcomes occuring before steroid use, and disregard the strong treatment-delay response relationship which is contradictory. Figure 24 shows analysis by strongyloides prevalence.
The third-party analysis that author references for the strongyloides theory is confounded by treatment delay — the high prevalence group has more early treatment trials, and the low prevalence group has more late treatment trials, i.e., the analysis reflects the greater efficacy of early treatment. More details can be found in the strongyloides section.
Author seems biased against believing any large effect size. We note that large effect sizes have been seen in several COVID-19 treatments approved by western health authorities, and also that better results may be expected when studies combine multiple effective treaments with complementary mechanisms of action (as physicians that treat COVID-19 early typically do).
Author is suspicious about a study based on the country of the researchers, and also appears biased against non-native speakers, with comments such as “unreadable” for one paper, compared to “written up very nicely in real English” for another.
Author calls a physician that has reported zero deaths and 5 hospitalizations with 2,400 COVID-19 patients “a crazy person” that “put his patients on every weird medication he could think of”.
Author disregards the dramatically higher mortality for Gamma vs non-Gamma variants (aHR 4.73 [1.15-19.41] [Zavascki]), instead concluding that higher mortality indicates fraud in one instance, while in another instance assuming that the related confounding by time in the Together Trial is not significant.
Author’s review of the 30 studies appears cursory, for example author appears unaware that the ivermectin dosage is very different in the ivermectin + doxycycline arm of [Ahmed].
Author refers to studies with positive but not statistically significant results as “negative” [Mohan], or “[the] original outcome would also have shown ivermectin not working” [López-Medina], which are incorrect conclusions [Amrhein].
Author appears to accept the analysis and accusations of GMK as correct, however that author is often incorrect.
Author is concerned that we detail problems with [López-Medina], while correctly noting that the outcomes in this trial are actually positive and in favor of ivermectin (while not statistically significant in isolation).
Author is concerned that we specifically comment on [López-Medina, Together Trial]. We note that it has been others that have focused on these trials — we comment on them because they have received special attention, including being held up as sole evidence overriding all other trials, despite having major issues.
Author claims that nobody can find issues with [Vallejos], which suggests that they have not read the study, or our analysis (hover over the reference and select “Notes”).
I want to respond to five parts of this.
First , the claim that I “[appear] to be against all treatments, labeling them all “unorthodox” and “controversial”, even those approved by western health authorities, including casirivimab/imdevimab, bamlanivimab, sotrovimab, and paxlovid.” They suggest I am turning my readers away from other treatments including ones that are already standard of care in western health systems.
This is false and I don’t know where they’re getting it from. Corticosteroids, fluvoxamine, and Paxlovid seem provisionally great. I haven’t looked into the monoclonal antibodies but if western health authorities say they’re fine I have no reason to doubt that. I even think there are plausible arguments (though no proof) for a few less-used options like zinc.
Obviously I urge my readers to get good treatments and not bad treatments. In fact, you even have my permission to pester your doctor about giving you a fluvoxamine prescription if you’re in the appropriate stage of COVID and they don’t think of it themselves. If they tell you it might have dangerous side effects, tell them that I have more experience with it than they do, and no it doesn’t (unless you are bipolar or in some kind of special bizarre high-risk category).
Second , they claim that I only looked at ivermectin for early treatment, and not for prophylaxis. This is true, and I agree a more thorough review would have analyzed the prophylaxis results too. I am not that thorough, and I assume that whatever is going on with the first 30 studies gives you a strong prior on what’s going on with the next 30. But they’re right that I didn’t prove it.
Third , the comments on my analysis. I agree with the ivmmeta people that I throw out many studies. I think this is correct, unless you also want to end up believing in psychic powers, stereotype threat, and social priming. The story of science over the past ten years has been learning that lots of studies suck and that we can’t draw conclusions until after eliminating the sucky ones.
Fourth , the comment on my biases. I am happy to own up to most of these. For example, yes, I am (slightly) biased against high effect size studies. See this article on Impossibly Hungry Judges for where I’m getting my intuitions on this. If you claim a very large effect size, it should be really obvious. If some studies show medium-low effect sizes and others medium-high, that’s within the range of normal variability and methodological disagreement and so on. If some studies show it cures literally everyone, and others show it does nothing whatsoever, then something has gone terribly wrong: maybe one group is making up data. If it’s a random sketchy guy who has a history of having made up data before (eg Carvallo) vs. huge trials run by legions of prestigious scientists, I’m going to assume it’s the first guy. This is especially true in the context of a few good ivermectin studies (eg Mahmud), which show that it has decent effect size like every other drug, but doesn’t cure literally everyone. Mahmud disagrees with the ones that find no effect, but it equally disagrees with the ones that find it’s a 100% perfect cure.
I am happy to own up to being biased against certain countries. I am not sure that the Egyptian scientific community has as strong an anti-fraud mechanism as some other places, given their history of fraudulent papers. I feel bad for innocent Egyptian scientists who might have a harder time getting people to take them seriously as a result, but not so bad that if an Egyptian paper comes up with results much better than everyone else, I’m not going to be suspicious.
Fifth , the comments on statistical technique. If I understand ivmmeta right, they want to think of every directionally-positive paper as “positive”, and every directionally negative paper as “negative”, without considering statistical significance, and are upset that I call not-statistically-significant papers “negative”. I think this only works if you have a very optimistic view of meta-analyses, which I do not, for reasons ivmmeta itself exemplifies. Ivmmeta links to some papers on abandoning the idea of statistical significance, which I think makes sense in some contexts, but the contexts are “you think two seconds about what you want to replace it with”, which I am not sure ivmmeta is doing here.
I actually think this might be more of a crux between us than anything about ivermectin itself. The same people behind ivmmeta have put up websites claiming that 19 different substances, including HCQ, testosterone-blockers, the spice curcumin, vitamins A, C, and D, etc, all cure coronavirus with pretty large effect sizes. I think this is because they are using a nonconventional form of statistics which is always going to find positive effects. I understand and respect why they’re doing this - they link eg this article condemning the idea of statistical significance, which makes good points. But you can’t throw it out without having a replacement. I think ivmmeta is trying to pioneer a new way of thinking about science and statistics without p-values, but I think its new way is actually bad and will get positive results almost all the time. I’ve seen a lot of fruitless debate between ivmmeta and doctors, but I wonder if you could have a fruitful debate between them and statisticians.
I’ve been thinking about this in the context about how ivmmeta does better and clearer science communication than everyone else. As the saying goes, “for every problem, there is a solution that is simple, elegant, and wrong”. The establishment takes a pile of garbage studies, throws lots of kludges and human judgment at it, and comes up with a result it’s not great at justifying but which is occasionally right. Ivmmeta is taking the same pile, doing a bunch of simple common-sense stuff to it, presenting it all in a natural and elegant manner, and is doomed to fail. We like to pretend that the scientific method and statistics and so on are objective, but right now the kludges and human judgment are doing most of the work, and when you take them out the whole thing collapses.
Alexandros Marinos is the most thoughtful and dedicated ivermectin proponent I know of. He’s been thinking a lot about my post, so far without any clear conclusions, but I’ve enjoyed reading his process, which has also led to helpful explainers like this one:
A few points of his I want to discuss in more depth:
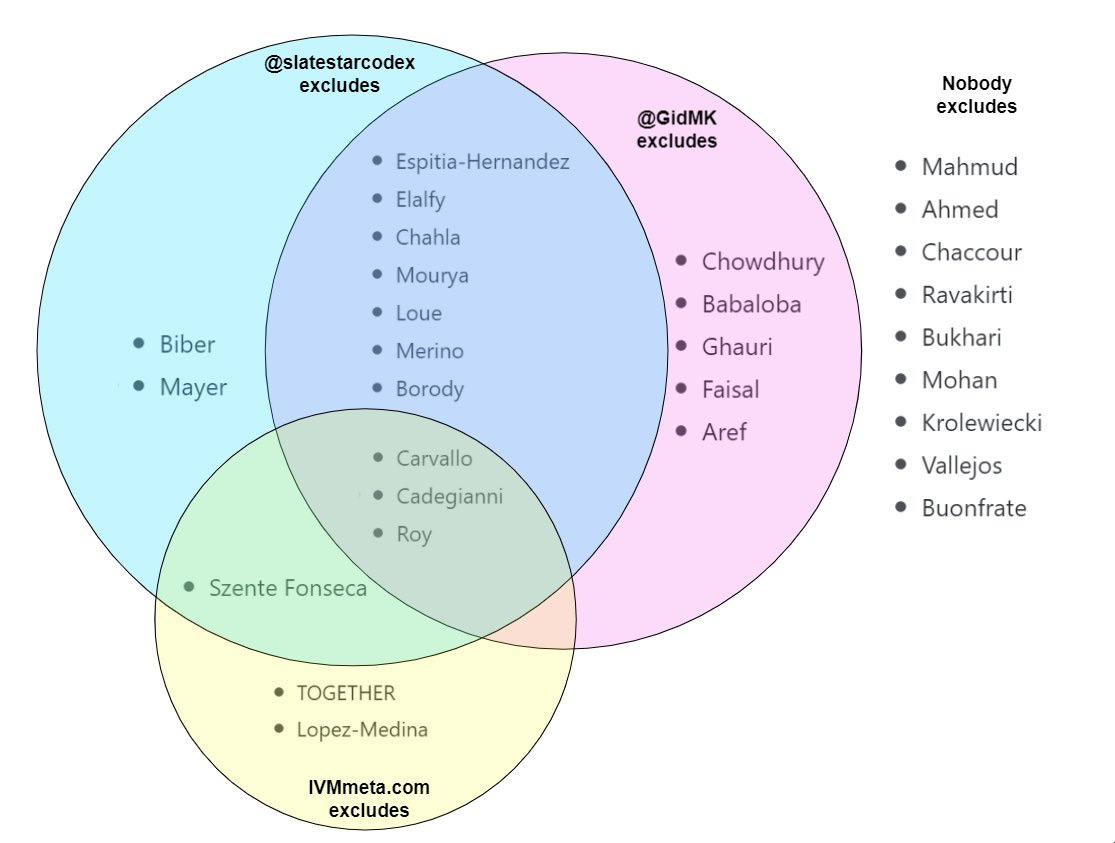
He’s interested in seeing what happens if we exclude or include different groups of things, which I support. I was hoping to try something like this before I realized how overwhelming doing just the stuff I did was going to be.
I think the main thing I want to cram into his head is how many pseudosciences that have to be false have really strong empirical literatures behind them. There are dozens of positive double-blind RCTs of homeopathy. I feel like I can explain what went wrong with these about a third of the time. The rest of the time, I’m as boggled as everyone else, and I just accept that the biggest studies by the most careful people usually don’t find effects, plus we should have a low prior on an effect since it’s crazy. This makes me pretty willing to shrug and say “Yeah, I have no idea what went wrong here, but a few big RCTs didn’t find an effect, plus I have a super-high prior for any new medical thing being false, so whatever, let’s move on”, which I admit is unvirtuous but I’m not sure how to avoid it.
But also:

I admit this is true and it sucks. I have no solution for it right now. I think of it as like the Large Hadron Collider. If the people who run the LHC ever become biased, we’re doomed, because there’s no way ordinary citizens can pool all of our small hadron colliders and get equally robust results. It’s just an unfair advantage that you get if you can afford a seventeen-mile long tunnel under Switzerland full of giant magnets.
I do think it’s occasionally possible to have genuine bottom-up medical research: ketamine seems to have worked this way. Even the trials that found fluvoxamine worked were funded by a random billionaire, which is sort of bottom-up in the sense of not being some established clique of experts with a vested outcome in the result. But I don’t think we know how to do this consistently yet, even though it would be cool if we could.
Lots of people were skeptical of the worms hypothesis. Rzztmass writes:
The worms thing is clever, but it doesn’t really work.
Hyperinfection syndrome is pretty rare. For it to make even the slightest dent in the numbers, you would have to assume very very high prevalence of Strongyloides and also far higher incidence of hyperinfection syndrome than what has been described.
Even if that were true, you would somehow have to reconcile doctors doing trials in countries where lots of patients have Strongyloides, where the doctors are familiar with steroids causing hyperinfection and then being fine with a trial arm risking to cause just that.
We are willing to accept fraud already and I consider fraudulent data to be more likely by far than doctors knowingly putting their patients at risk of dying just for nice looking data.
The more realistic stance though is that death or worsening due to hyperinfection is a rather rare outcome and doesn’t influence numbers significantly. That’s why the doctors in those countries went along with a study that would otherwise be unethical. I still don’t know where the significance comes from, but it’s not strongyloides hyperinfection.
Something like this was also the objection of Bret Weinstein, a biologist, podcaster, and author who’s been another big ivermectin proponent:
 Bret Weinstein @BretWeinstein@Ravarora1 @coldxman @PierreKory A substantial piece of work that crashes and burns with a deeply suspect ad hoc hypothesis in need of a test. cc: @slatestarcodex, @alexandrosM[4:01 AM ∙ Nov 19, 2021
Bret Weinstein @BretWeinstein@Ravarora1 @coldxman @PierreKory A substantial piece of work that crashes and burns with a deeply suspect ad hoc hypothesis in need of a test. cc: @slatestarcodex, @alexandrosM[4:01 AM ∙ Nov 19, 2021
154Likes5Retweets](https://twitter.com/BretWeinstein/status/1461545144868507648)
I agree this is speculative and not yet tested by formal studies, which was why I only gave it ~50% confidence in the summary at the end of my post.
(I also am kind of embarrassed because I think I failed to emphasize enough that I didn’t invent this hypothesis. Credit and/or blame should go to Drs. Avi Bitterman, David Boulware, and the many people who have published work on treating COVID in parasite-filled areas)
But a few points:
Although strongyloides hyperinfection is a particularly obvious way worms can be bad, it’s probably not the main one. There are lots of kind of worms that can be bad in lots of kinds of ways.
But I’m also not as skeptical as Rzztmass. We don’t have to speculate about whether doctors in parasite-prone areas would give steroids - we know they did! Dr. Bitterman asked and lots of these trials admitted giving steroids to their patients. Ravakirti gave steroids to the entire control group, Lopez-Medina gave it to some controls. It happened! We know it happened!
But even strongyloides itself isn’t actually that uncommon. In Bangladesh, where some of the best positive trials come from, seroprevalence is 5-22%. And in Ravakirti, one of the studies in East India (which I assume is similar), got corticosteroids.
The entire ivermectin advantage in Ravakirti et al comes from 4/50 people dying in the control group compared to 0/50 in the experimental group. If they have 10% strongyloides prevalence and half of infected people who take steroids get a bad reaction, that explains half of the effect. The other half could be coincidence / other worms / I’m underestimating the effect of strongyloidiasis / real positive effects of ivermectin, but I don’t think the effect of strongyloides is obviously of the wrong magnitude to matter here.
See further discussion by Dr. Bitterman here and here..
By the way, the strongyloides hypothesis made it into the Economist here.
GeriatricZergling writes:
My other replies are scattered all over the place, so I’ll just add this as a top level comment, pertaining the the general point of “parasites fucking with your immune system even without clinical hyperinfection”.
From Weatherhead & Mejia 2014, who are themselves reviewing this stuff before delving into hyperinfection:
“The host innate and adaptive immune response plays a critical role in the maintenance of chronic strongyloidiasis and the prevention of hyperinfection syndrome and dissemination. Similar to other helminth infections, strongyloidiasis elicits a Th-2 lymphocyte predominant immune response with production of cytokines, IgE antibodies, eosinophils, and mast cells which participate in expulsion and killing of the helminth [3, 7, 11]. Strongyloides antigens activate eosinophils via the innate immune response [12]. Activated eosinophils act as antigen presenting cells to stimulate antigen-specific Th-2 cytokine production including IL-4 and IL-5 [8•, 12]. IL-4 induces activated B lymphocytes to class-switch for production of IgE and IgG4 antibodies and additional cytokines (IL-8) attract granulocytes such as neutrophils to aid in larvae killing [7, 11, 12]. IgE production allows for mast cell degranulation and enhances further eosinophil migration [8•]. IL-5 acts as an eosinophil colony stimulating factor promoting further eosinophil growth and activation [8•, 11, 12]. Approximately 75 % of patients with chronic strongyloidiasis have peripheral eosinophilia or elevated total IgE levels [4, 12]. Protective immunity to infective larvae has been found to involve specific Strongyloides antibodies, complement activation and neutrophils in antibody-dependent, cell-mediated cyotoxicity type responses [11]. Patients with severe disease have been shown to have a significant decrease in antibody levels and a decrease in eosinophil level compared to asymptomatic infected individuals, suggesting that both antibodies and granulocytes play a significant role in protection from infection [11]. The sophisticated interaction between strongyloidiasis and the host immune system allows for long-term survival of the pathogen in the host gastrointestinal tract.”
Note again that this is describing the effects of normal, run-of-the-mill strongyloidiasis in immunocompetent patients ; literally the next sentence after my quote ends starts talking about what happens when the patient’s immune system starts being suppressed or otherwise behaving abnormally for other reasons.
As I mention elsewhere, immunology is literally the part of biology I’m worst at, and my knowledge comes from a “host-parasite-evolution” background instead, so I cannot translate this into anything clinical. But what it does show is that the specific parasites affected by ivermectin will impair the host immune system in a variety of ways even at normal, non-hyperinfection levels, and this is a typical thing for strongyloidiasis. This, in turn, is strong evidence for the overall hypothesis of “COVID + strongyloidiasis is worse than regular COVID, so killing the worms should help.”
On the other hand, there’s some speculation that having some kinds of parasitic worms might help COVID. Remember, a lot of COVID deaths are because your immune system over-reacts and causes too much collateral damage; this is why immunosuppressants like corticosteroids are so useful. But parasitic worms are constantly trying to sabotage your immune system to prevent it from killing them, so people with chronic worm infections are already a little immunosuppressed, which is probably good for them. Probably the exact good/bad balance depends on the specific worm, infection, and person involved.
gettotea writes:
I agree. Scott needs to factor in regional prevalence. Trials are run in more sophisticated cities, where prevalence of worms would be far less than the outskirts. I live in Chennai, India, and prevalence of worms would be orders of magnitude away from a randomly picked village in India.
Trials are also run in pretty well funded hospitals, which again naturally have a self-selection for wealthier people who again will be far less likely to have worms.
Mahmud et al was run in Dhaka, which was where my former 5-22% strongyloides number was taken from - 22% in the slums, 5% elsewhere.
Ravakirti et al was run in Patna. I can’t find strongyloides prevalence numbers there, but this study says 63% of people there have at least one intestinal parasite.
Also, I have spent approximately two hours in Patna, and although I mostly stayed in the bus station, I still got a very strong “probably full of parasitic worms” vibe from the place.
The TOGETHER trial was a very large and official study that was pessimistic about ivermectin working. We still don’t have the full paper, but ivermectin proponents are skeptical partly because of a possibility that the treatment and control groups entered at different times. This could potentially confound the study since differently-severe variants were entering the country. But James Watson writes:
I don’t think that it is correct that they used non-contemporaneous controls for the ivermectin TOGETHER study. This is a well-known problem in adaptive trials where new arms can enter and leave the platform. The controls that they will have used are only those who could have been randomised to ivermectin. See for example their write up of fluvoxamine (https://www.thelancet.com/journals/langlo/article/PIIS2214-109X(21)00448-4/fulltext)
He also adds:
Regarding fluvoxamine: interesting that your assessment is that it “works”. From a Bayesian perspective, a priori it’s highly unlikely to do anything (some random doc decided to test because why not; no known mechanism of action); and there is a real problem of post-randomisation bias. See this article for more detail https://www.the-scientist.com/news-opinion/a-closer-look-at-the-new-fluvoxamine-trial-data-69369
Huh, I’d heard it’s a sigma receptor agonist, which decreases immune system overresponse, which is probably what we want. I agree people thought of this post-hoc, but it’s not a terrible explanation.
…though it’s possible I’m overstepping my expertise here to someone who knows much more than I do, since I notice the statistician and trial design expert quoted in that Scientist article is also named…James Watson. Hopefully he isn’t also the DNA guy or I’ll be totally out of my league.
Moving to the more political sections, The-Serene-Hudson-Bay writes:
I think also missing is the behavior of conservative political and media elites, who are actually in a social class where they might have immunologist relatives but who kept up anti-blue tribe COVID skepticism. Trump is vaccinated, Fox News has an internal vaccine passport system, these are the people best positioned to persuade skeptics motivated by ‘hostile aliens’ and they refuse to do it because maximal ongoing culture war serves their interests.
Many people said something similar. I’ll admit I’m confused what’s going on here. Articles like Trump Booed In Alabama After Promoting COVID Vaccine make me think that the conservative elites know it works, have gotten vaccinated, briefly tried recommending this to their constituents, learned their constituents didn’t like this, and since then have been awkwardly punting questions about it.
The conservative elites backing off doesn’t seem to require an interesting explanation - yeah, populists will drop positions that the populace turns out to hate. So the interesting question is why the (conservative) populace hates it so much, which is what I tried to speculate on.
I also think people are overestimating conservative elites’ role here by deliberately conflating opposition to vaccine mandates with opposition to vaccines. A lot more elites have come out in favor of the first than the second.
The people on Hacker News were extremely kind to me. csee wrote:
While reading this piece I got a little depressed that most journalism is just such utter trash compared to it. I’ve read so many articles on ivermectin and none of them gave me even ten percent of the clarity that this article gave me. Can you imagine if writing and journalism of this calibre was commonplace among practising “journalists”? And look at how this piece compares to the CDC’s and WHO’s science communication. It’s a shame that clear thinking and communication is so scarce.
nonameiguess responded:
While Scott has a pretty decent natural talent for writing, he also has a MD, he’s a board licensed practicing psychiatrist who has been working for a decade in the field, and he has spent at least the last twenty years gaining a pretty decent broad exposure to statistical and research methods. I don’t believe he disclosed what Substack paid him, but he is in the “paid tier” and has said it was a mistake to even agree to that because the subscriptions he has gotten exceed what Substack paid him. In short, if you want most journalism to hire licensed medical doctors with decades of experience in science and statistics, and natural writing talent on top of that, expect journalism to get a lot more expensive. A market certainly exists for Scott, but I’m not sure the market exists for all journalists to be as highly qualified as Scott. Or, for that matter, even for CDC and WHO PR arms. They definitely aren’t paying their communications officers whatever Substack is paying Scott, or probably even what his psychiatry practice is paying him.
I’m not publishing this exchange just because I like compliments, I actually have a relevant story here. When I was working on the ivermectin post, I mentioned it to a friend who’s a journalist. She shocked me by reciting a list of all the same studies I’d been looking at, her (completely correct) opinion on each, and then ending with the same conclusion I did (any remaining positive signal after you remove the fraudulent studies might be because of worms). I asked why her article hadn’t said any of this. She said that, in consultation with her editor, they decided that reviewing all the studies would have taken too much space, and mentioning the worms would have been too speculative.
I was flabbergasted. I thought I was doing some pretty novel journalistic research here, better than all the other science communicators, but here I was just lucking out by not having an editor telling me to maintain normal journalistic standards of concision and evidence. I think this journalist was very unrepresentatively good - but it was still a bit of a wakeup call.
My biggest advantages over many articles that were less comprehensive than mine were having Substack - a great platform that lets me publish whatever I want - and even more important, having all you excellent readers who are masochistic enough to read ten thousand word essays speculating about intestinal parasites. So thanks for that, and give journalists a break.
(except of course the New York Times. Ecrasez l’infame!)
In response to a request to hear a vaccine skeptic’s perspective, Tophattington writes:
I am not a vaccine sceptic, I simply refused to take them as one of the few means I have available to protest against lockdowns, particularly as the government here [UK] used covid-19 as an excuse to arrest well over a hundred political dissidents in a single day. This became more strident as I oppose the way that lockdowns and other restrictions have created an element of duress to taking medical treatment, and also the way regions of the country have set up systems specifically intended to discriminate against unvaccinated people.
To mandate vaccines is to state that humans are all born defective, and only become non-defective after jumping through state-approved hoops. It is philosophically corrosive to everything I believe in. It’s the kind of thing that the avant-garde of progressivism would have called “biopower” before they conveniently forgot about the subject in 2020.
The hostile alien analogy is missing a key part in all this. The hostile actions aren’t far in the past, but instead began in March 2020 with lockdowns, and remain ongoing. The moment governments around the world granted themselves unchallengeable authority over the minutia of private life, and placed their entire populations under house arrest, the growth of opposition to vaccination became inevitable. This is real, serious harm, inflicted upon billions. It’s a scale that I still struggle to wrap my head around.
As the entire visible medical establishment fell in line with this power-grab, I consider them untrustworthy too. How can I believe that the average doctor cares about my health when the average doctor was happy for the British regime to abuse me like this? But I have enough skill to just read the vaccination study results myself and see that it’s effective but not effective enough to leave the regime with no excuses to continue restrictions. That’s all that ends up separating me from an active opponent to vaccination.
This is why opponents to lockdown and opponents to vaccination overlap. Despite claims that this is illogical because vaccines are a way to end restrictions (they’re not, and Europe is currently proving this, Gibraltar most notably). Sure, this means I have some strange allies, but to crib off something that probably wasn’t said by Muhammad Ali: No anti-vaxxer ever locked me down.
I kind of sympathize with this (and am considering refusing the booster to protest them not sending spare doses to the Third World), but refusing to get vaccines seems like the most counterproductive way to protest lockdowns. Not only will it ensure the lockdowns last longer (because there are more cases), but it’ll just provide pro-lockdown people with an easy opportunity to tar all their opponents as science deniers.
I guess it depends whether you trust people that vaccines will at least slightly reduce cases, and that reductions in cases will lead to fewer lockdowns. I think it’s easy to get discouraged about this given the many “okay, in just a few weeks this will all be over and we can reopen for real” bait-and-switches, but in the long run I do think we’ve gotten less locked down as case numbers have declined. I don’t know how much of that has been epidemiologists agreeing the crisis is less severe vs. anti-lockdown activists forcing governments’ hands.
And all of this is here in the US. I understand a lot of other places are having some really weird experiences right now, and I hope everyone’s okay.