Know Your Amphetamines
In the 1950s, a shady outfit called Obetrol Pharmaceuticals made a popular over-the-counter diet pill called Obetrol. If you’re familiar with any of: the 1950s, shady pharma, or diet pills, your next question will be “did it contain amphetamines?” and the answer is yes, loads of them. Obetrol was a mix of four different amphetamine salts: racemic amphetamine sulfate, dextroamphetamine sulfate, methamphetamine saccharate, and methamphetamine hydrochloride. Why did they need four different kinds of speed? I’m not sure. The uncharitable explanation is: for the same reason Dr. Nick’s Cure-All Home Remedy has twelve different herbs, ie customers think things with more ingredients are better.
By the 1970s, people figured out meth was bad, so Obetrol replaced their two methamphetamine salts with two more kinds of non-methylated amphetamine. But the FDA continued to crack down, and although the historical paper trail goes kind of dark, it looks like Obetrol had disappeared by the 1980s.
As usual in pharma, someone bought Obetrol Pharmaceuticals, then someone else bought them , and after a few iterations of this, all their intellectual property ended up with a company called Richwood. They decided to rebrand Obetrol as “Adderall “ and pitch it as an ADHD cure.
Treating ADHD with amphetamines was hardly a new invention. Psychiatrists had been doing it since the 1930s, albeit with slightly different drugs. Remember, many organic chemicals come in two versions, a “right-handed” or “d” version and a “left-handed” or “l” version. Benzedrine (a 50-50 d/l split) and Dexedrine (pure d-amphetamine) were the treatments of choice throughout the mid-20th century. So why was it Adderall - a weird combination of four different salts selected kind of at random by a sketchy diet pill company - that caught on?
I’m not sure. My best guess is good timing plus good advertising. In the early 20th century, ADHD was called “minimal brain dysfunction” and diagnosed only in the most extreme cases. A few children with absolute and total inability to function at all got diagnosed and given Benzedrine or Dexedrine; everyone else was left to fend for themselves. As far as I know, this wasn’t because doctors had a principled commitment only to diagnose extreme cases - I found a paper from 1975 arguing that up to 5 - 10% of children probably had minimal brain dysfunction, the same number estimated to have ADHD today. Parents just didn’t know about it and didn’t really have “take my kid to a psychiatrist” in their set of plausible options to consider.
In the early 1990s, psychiatric research, a series of popular self-help books, and the business interests of Richwood Pharmaceuticals all converged on the idea that it was important to get more people diagnosed with ADHD. Adderall entered the market at exactly the right time, and it became everyone’s go-to ADHD medication.
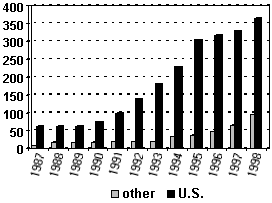
US Ritalin consumption in millions of doses/year, probably a good proxy for number of ADHD diagnoses, approximately septupled during the 1990s (source)
Even if we agree that amphetamines are the right treatment for ADHD (many people don’t!), how concerned should we be that the particular amphetamines we use are a random mix of salts selected by sketchy 1950s diet-pill peddlers? Dexedrine is an older formulation with pure d-amphetamine (sulfate). No l-amphetamine, no weird combination of salts. Should we just use that?
This is hard to study, because it’s not obvious how to dose both medications. If we start out suspecting that both isomers are equally strong, we might dose 10 mg of Dexedrine vs. 10 mg of Adderall. But in fact we have reason to think that d-amphetamine is a bit stronger, so maybe 7 mg of Dexedrine vs. 10 mg of Adderall? But then any difference we find might just be a question of choosing the wrong doses rather than a real distinction.
Arnold, Huestis, and Smeltzer, 1976 and Gross, 1976 compare pure d-amphetamine to a mix of d and l amphetamines. Both studies find that both d-amphetamine and l-amphetamine are effective stimulants, but that d-amphetamine seems to work better for most people. A rat model also finds some modest superiority for d-amphetamine, showing that both isomers improve attention, but d-amphetamine additionally improves hyperactivity and impulsivity.
Is there any advantage at all to including l-amphetamine? AHS find that a small subgroup of patients seem to do better on it, but this is a study from 1976 and honestly I don’t trust them to find small subgroups responsibly. And Gross finds that some people have fewer side effects on a mix of both than on d-amphetamine alone. This is a bit strange - shouldn’t two chemicals have more side effects than one chemical? My guess is that d-amphetamine is just stronger, and so people getting their amphetamines as a mix of a strong chemical and a weak chemical are effectively on a lower dose and get fewer side effects.
James et al switch children back and forth between Adderall and Dexedrine to see which works best. They find the winner changes from measure to measure. But the tiebreaker was just asking the teacher which week the child seemed to be doing the best work in class, and the teacher chose a Dexedrine week almost twice as often as an Adderall week.
Joyce, Glaser, and Gerhardt claim to find that Adderall creates stronger and more prolonged changes in dopamine release than other amphetamines. But they use a bizarre dosing regimen which equates 0.5 nmol Dexedrine, 0.68 nmol Adderall, and 1 nmol racemic amphetamine as “identical doses” of each, based on a theory that l-amphetamine has no independent action but just modulates d-amphetamine. As far as I can tell this is totally false, and their study contradicts everything else I know, so I am going to nervously ignore it for now.
What about the evidence from patient ratings? Online databases contain several thousand of these…
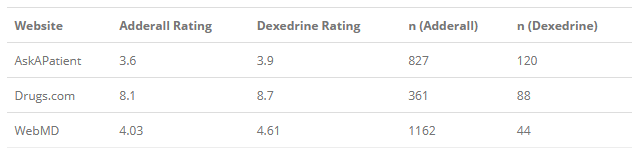
…and they pretty conclusively show that on average patients prefer Dexedrine to Adderall. This is unblinded and uncontrolled, we don’t know what dose any of them were on, and patients sometimes like addictive medications that aren’t very good for them by normal medical standards. But again it seems like a pretty resounding victory for Dexedrine, which is what I’d expect. Honestly it’s pretty weird that our go-to ADHD medication includes four random salts and a bunch of l-amphetamine when a pure d-amphetamine medication we could use instead is right there.
I do appreciate Dr. Charles Popper’s contribution here; he notes that since Adderall has so many different salts, they take different amounts of time to get absorbed by your body, which means Adderall has a more gradual onset and offset compared to something purer like Dexedrine. Things with gradual onsets and offsets are probably less addictive and less likely to produce withdrawals and “crashes”. As far as I can tell, this is the strongest pro-Adderall argument.
Vyvanse is the newest and most expensive member of the amphetamine stimulant family. It’s lisdexamphetamine - ie Dexedrine attached to a random inactive molecule called lysine. As long as the lysine is attached, it can’t stimulate anything. The body removes the lysine at a slow, consistent rate, which means that you get a slow, consistent release of stimulant into the bloodstream. This is advertised as especially good for people who are worried about addiction. It’s hard to abuse or overdose on Vyvanse; no matter how much you take, your body will still only activate it at the same, slow rate.
My patients love Vyvanse. I try hard to convince people to take older, less expensive medications unless they’re absolutely sure that the newer flashier one works better, but my patients are very convinced Vyvanse works better than Adderall. I used to think this was because something about the complicated timed release mechanism makes it “smoother”. This is definitely what the pharma company that designed it wants me to think, and I admit there is some evidence for it.
But one neglected perspective is that once you take away the lysine, Vyvanse is basically Dexedrine, not Adderall. Almost everyone likes Vyvanse better than what they were taking before. But usually they were taking Adderall before. If Dexedrine is really better than Adderall - and common sense and the patient rating websites say it is - then that goes some of the way to explaining Vyvanse’s superiority before we even get to the complicated timed release stuff. Pharmaceutical companies are always trying to re-release old medications in ways that bamboozle you into thinking they’re new medications, so they can charge more money for them. In this case they did so good a job that I honestly can’t tell if that’s what they’re doing or not.
Evekeo takes Adderall’s questionable decision to include l-amphetamine and doubles down on it. Remember, Dexedrine is 100% d-amphetamine and Adderall is 75% d, 25% l. Well, Evekeo is 50-50. This should make it strictly worse than Adderall, and my patients’ feedback seems to agree with this. The supposed point of making it is those studies that show a small subgroup of people seem to get some extra benefit from l-amphetamine. The real point of making it is probably as a me-too drug; it doesn’t require any research, since l-amphetamine and d-amphetamine have both been around forever, but since it’s new and different you can charge a lot of money for it.
I can’t think of any situation where it would be reasonable to prescribe Evekeo as a first-line stimulant. If someone has done sort of okay on Adderall but has lots of side effects, and you put them on Dexedrine and they get worse instead of better, I suppose you could try putting them on Evekeo to see if they really are in the small subgroup of l-amphetamine beneficiaries. I’m just annoyed that this relatively rare legitimate use case serves a fig leaf for the inevitable Big Pharma campaign to push this new on-patent very expensive medication on a bunch of people who don’t need it.
Desoxyn is the undisputed king of the patient rating websites. Here’s the same graph as before, except I’ve added Desoxyn to the last column:
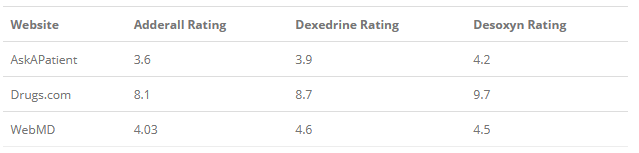
These are some amazing numbers. Adderall itself usually has one of the highest ratings of the thousands of drugs on the site, Dexedrine beats Adderall handily, and Desoxyn wipes the floor with Dexedrine (except on WebMD, which has the smallest sample size). This drug is getting ratings that shouldn’t even be possible. And the patient summaries are in line with this - here are a few:
I have been on every derivative and variation of stimulant, SSNRis SSRI, Tricyclics, beta blockers and all sorts of combinations of above and never have come across such an amazing compound. as Desoxyn. I think that there is a definable difference in mood thoughts and the way thoughts flow with memory and with present day crises.
And:
After dealing with depression and ADD for most of my life, and having tried literally every conventional anti-depressant and ADD medication, I can honestly and without hesitation say that Desoxyn is the absolute best medication I’ve ever used to treat my ADD.
And:
How is this not more widely prescribed? My doc had me on Strattera at first, didn’t help at all. Next I switched to Concerta, which worked, but increased my anxiety, and I had a crash. Next I switched to Adderall, which had almost the same effect as Concerta but on top of that I had no appetite. Finally I switched to Desoxyn and that’s when my life started to turn around. My grades instantly went up and homework became fun for me. Math problems became like a puzzle, and history became fun, like watching a real-life movie. Right when I made the switch to Desoxyn, I got caught up on ALL my homework and my grades instantly switched from D’s and F’s to B’s and A’s. Not only that, but my social anxiety was completely GONE.
All the reviews are like this. And I bet all of these patients are telling the truth. Sometimes I read drug reviews and I wonder whether these people are special cases, or driven to exaggerate, but these descriptions match my impression of how the average Desoxyn patient feels.
What’s the catch? Desoxyn is methamphetamine. The FDA and DEA discourage doctors from prescribing it, but it’s still technically legal with an MD’s prescription, and there are still some doctors who will use it for the most refractory cases. It is officially indicated for ADHD and obesity (really!), but gets used off-label for narcolepsy and various sleep disorders.
There’s a lot of confusion around the difference between amphetamine and methamphetamine. On the one hand you have anti-psychiatry activists who will say that using Adderall for ADHD is exactly like giving kids crystal meth; on the other you’ll have people who say that obviously normal amphetamine is okay, but meth -amphetamine is a demonic substance that will hijack your brain and destroy your life. The truth is more complicated.
Methamphetamine crosses the blood-brain barrier more effectively than unsubstituted amphetamine, but I’m not sure how much that matters since people take different doses of both, and a high dose of unsubstituted will end up with more reaching the brain than a low dose of meth. It seems to inhibit the dopamine transporter more effectively, which might matter, but I’m not enough of a pharmacologist to know how much. Meth takes effect more quickly, which seems to increase addictiveness in a sort of behaviorist sense where the sooner a stimulus gets reinforced, the more rewarding it will feel. If all of this sounds kind of weak to you, you’re not alone. Shoblock et al write:
Despite the repeated claims of METH being more addictive or preferred than AMPH, proven differences between METH and AMPH in addiction liability and in reward efficacy have evaded researchers. Animals self-administer METH and AMPH at comparable rates (Balster and Schuster 1973) and humans prefer similar doses (Martin et al. 1971). Also, neither humans nor animals discriminate between equal doses of METH and AMPH (Huang and Ho 1974; Kuhn et al. 1974; Lamb and Henningfield 1994). Furthermore, while METH is commonly believed to be a more potent central psychostimulant than AMPH, no direct comparison on the potency of the two drugs to stimulate central processes have been verified. In addition, no previous study has directly compared the acute effects of the two drugs on locomotor activity, an important central process that contributes tothe definition of psychostimulant. Moreover, there are no known neurobiological differences in action between METH and AMPH that would account for the putatively greater addictive, rewarding, or psychomotor properties of METH.
I think there’s been a little bit more research since then, but the general takeaway - that the science doesn’t support the vast gulf between these two drugs in the popular imagination - still seems true.
What’s going on? I think addicts use meth very differently from the way generally responsible ADHD patients use amphetamine. It’s weirdly hard to find good data on methamphetamine route of administration, but this study shows that about 60% of users inject it, 23% snort it, and 52% smoke it - also, see this paper about “the second case of rectal methamphetamine abuse in the literature”. Route of administration makes a really big difference in how addictive and dangerous a drug is (see eg crack cocaine vs. regular cocaine), and I think this is a big part of the difference between seemingly okay Adderall users and very-not-okay meth users.
But maybe even bringing up route of administration is getting too complicated. The simplest explanation of the difference between meth users and responsible amphetamine users is that the meth users take much, much more. This study asks abusers how much they use in an average day, and gets numbers from about 300 to 800 mg. An average clinical dose of either Adderall or Desoxyn would be about 20 mg a day.
So abusers are taking about 25x a normal dose, and are usually snorting or injecting it. I think this explains the lion’s share of the difference between “methamphetamine abuse” and “responsible Adderall use” without having to appeal to chemical differences between meth and unsubstituted amphetamines. Those differences do exist, and they’re one reason why drug abusers prefer the methylated version. They’re just not as dramatic as you would think from seeing a successful college student on Adderall vs. a toothless vagrant on meth.
All of this would seem to suggest that doctors should be less scared of prescribing Desoxyn - except that if it were true, Desoxyn wouldn’t have as big an advantage over Adderall as the ratings suggest. I’m not sure what’s going on here. Maybe this is just the effect of the small but real advantages in BBB penetration and level of dopamine transporter inhibition. Or maybe it’s at least partly placebo - an ADHD patient whose doctor gives them meth feels like they’ve been allowed to dabble in forbidden magics, and is properly grateful in a way that makes them feel like their medication is more effective. I’m not sure. I only have secondhand accounts to go on - I’m too much of a wuss to prescribe Desoxyn myself.
When I treat ADHD with amphetamines, I usually start with Adderall/extended release Adderall, even though realistically Dexedrine would probably be an equally good or better choice. If it’s not working very well or there are too many side effects, I switch to Dexedrine/extended release Dexedrine. If Dexedrine doesn’t work because it seems too strong or the patient “crashes” too hard afterwards, or if I’m worried the patient is at risk of addiction, I will try Vyvanse (or some other solution to stimulant “crashes”); if Dexedrine works less well than Adderall and I am very confused and the patient is in an experimenting kind of mood, I might try Evekeo. If none of these work, a braver person than I am might try Desoxyn. As for me, I give up on amphetamines and start looking at Ritalin, modafinil, or other options.