Replication Attempt: Bisexuality And Long COVID
I learned from Pirate Wires that CDC data show bisexuals were about 50% more likely than heterosexuals to report long COVID.
Is this just because more women than men are bisexual, and more women than men get long COVID? Not exactly; in the data they cite, women (regardless of sexuality) have an 18% rate, and bisexuals (regardless of gender) have a 22% rate.
(aren’t all these numbers really high? You can find almost any number depending on how you ask the question; questions along the lines of “have you had any persistent symptoms including fatigue, brain fog, shortness of breath, changes to taste/smell, etc, etc, etc, since having COVID?” tend to produce numbers from 20-30%; most will say this symptoms are mild and don’t affect their functioning very much)
This seemed weird enough that I wanted to try replicating it with the ACX survey data (read more about the ACX survey here).
 The questions
The questions
I got much lower rates of Long COVID than the CDC, more like 3% than 20%. This isn’t surprising; ACX readers are mostly male (women get more long COVID), mostly young and healthy (older, unhealthy people get more long COVID), and I asked a stronger question (asking if you “have” “long COVID” sounds more definite than just asking if you have a few lingering symptoms).
Here are ACX rates by gender by sexual orientation:
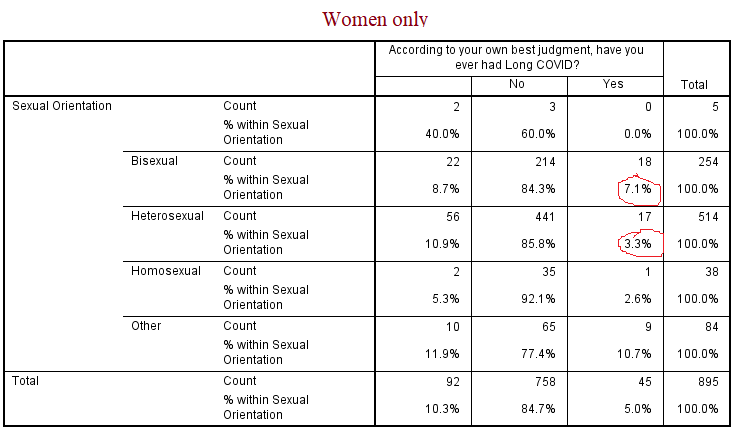
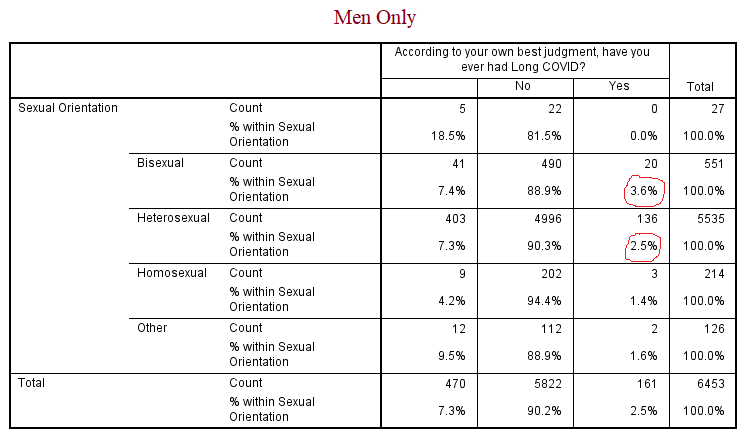
Bisexual women got long COVID about twice as often as straight women (though straight women were somewhat more likely not to respond, and if some of those nonresponses were people not wanting to admit long COVID, that could be a confounder). Bisexual men got long COVID about 50% more often than straight men. The female difference was significant (p = 0.02) and the male difference marginally significant (p = 0.08) on chi-squared tests.
Bisexuals and heterosexuals seem much more likely to be psychologically different than immunologically different, so I think this is a signal that a substantial percent of long COVID is psychosomatic.
Mental illnesses tend to cluster together, and people with diagnosed mental illnesses tended to have high rates of long COVID too. Limiting all analyses to men (to remove gender as a confound; there were many more male than female respondents), anxiety increased the risk of long COVID by a factor of 1.5, and depression by a factor of 2. Borderline personality - which classically is most associated with suggestability and a tendency towards culture-bound mental illnesses, increased the risk by a factor of 10 (albeit with small sample size: 3 of 13 male borderlines had long COVID).
Still, I find the bisexuality result most interesting. Depression and long COVID could correlate through “how likely is this person to medicalize the way they feel?” or “how likely is this person to admit their medical problems on surveys?” I can’t think of a good explanation for bisexuality, other than the obvious one; bisexuals have higher rates of most mental illnesses, therefore some long COVID must be a mental illness.
(Why does homosexuality, which also has increased rate of many mental illnesses, show so much less of a signal than bisexuality? I don’t know, and it’s a weakness of this theory.)
Last time I wrote about this, I said that some cases of long COVID were probably psychosomatic, but the majority weren’t. These new data don’t technically disprove that; bisexuals aren’t a majority of anything. But the signal here is strong enough that I’m going to walk my previous statement back and be much less sure that there aren’t a lot of psychosomatic cases (I still think most likely some cases are organic, just because you usually need a few organic cases to seed psychosomatic conditions, and there’s no reason why a serious and novel virus shouldn’t cause occasional post-viral syndrome).
If this were true, we could think of the excess psychosomatic cases of long COVID as a culture-bound mental illness, and consider compassionate treatment for the organic and unavoidable psychosomatic cases - alongside unawareness campaigns aimed at minimizing avoidable psychosomatic ones.