Sleep Is The Mate Of Death
Melancholic depressive patients report that they feel worst in the morning, just after waking up, get better as the day goes on, and feel least affected in the evening just before bed. Continue the trend, and you might wonder how depressed people would feel after spending 24 or 36 or 48 hours awake. Some scientists made them stay awake to check, and the answer is: they feel great! About 70% of cases of treatment-resistant depression go away completely if the patient stays awake long enough. This would be a great depression cure, except that the depression comes back as soon as they go to sleep. There’s a lot of great work going on to figure out how to make cure-by-sleep-deprivation last longer - see the Chronotherapeutics Manual for more details.
But forget the practical side of this for now. It looks like sleep is somehow renewing these people’s depressions. As if depression is caused by some injury during sleep, heals part of the way during an average day (or all the way during an extra-long day of sleep deprivation) and then the same injury gets re-inflicted during sleep the next night.
I think this is the position that Rantamäki and Kohtala are taking in their Encoding, Consolidation, and Renormalization in Depression: Synaptic Homeostasis, Plasticity, and Sleep Integrate Rapid Antidepressant Effects and several million other equally long and nearly-unreadable review articles.
R&K start by reviewing the synaptic homeostasis hypothesis of sleep developed by neuroscientist Giulio Tononi (equally famous around these parts for his integrated information theory of consciousness, see eg Scott Aaronson’s discussion here). As you learn stuff throughout the day, your brain builds new synaptic connections representing what you learned. For example, as you read this article connecting depression and sleep, your brain might be forming new synapses between neurons storing information about these two concepts (or strengthening existing synapses). That means as time goes on your brain will get more and more synapses, the synapses will become stronger and stronger, and everything will be more and more connected to everything else. But synapses take lots of energy to maintain. And “everything is maximally connected to everything else” works well for conspiracy theorists and Zen masters, but less well for neural networks trying to perform specific computations.
So you want to do what the AI people call “renormalization”. You scale down all your weights by some function, until they’re a set of smaller weights that represent the same information. For an oversimplified example, if you have three synapses with weights 90, 50, and 30, you can divide all of them by 100 to get 0.9, 0.5, and 0.3; the ratio between them is still the same. If the brain does this regularly, it can keep learning new information and keep the same average number/strength of synapses over time.
You can’t renormalize while the network is running; you want to turn it off first. Tononi thinks this is the point of sleep. You turn off the network. You send a bunch of brain waves through to figure out average synapse level. Then you gradually downgrade and prune synapses until they’re back at your set point. He cites lots of research showing that people gradually accumulate more and stronger synapses during the day, then lose them again during sleep, plus lots of reasons to think that the processes that happen during sleep are the sort of processes that would renormalize synapses.
Meanwhile, a different line of research has been suggesting that depression probably involves a deficit of synapses. For some reason the depressed brain is just really underconnected. People’s brains are smaller when they’re depressed, then get bigger again when they feel better; number of neurons almost never (maybe literally never?) goes up, so this is probably about the number/size of synapses. Also, the depressed brain uses less glucose, which we already established was a potential consequence of fewer synapses. Also, someone recently invented a complicated way to measure synapse density directly using radioligands and MRI, and preliminary studies show it’s pretty highly correlated with depression severity.
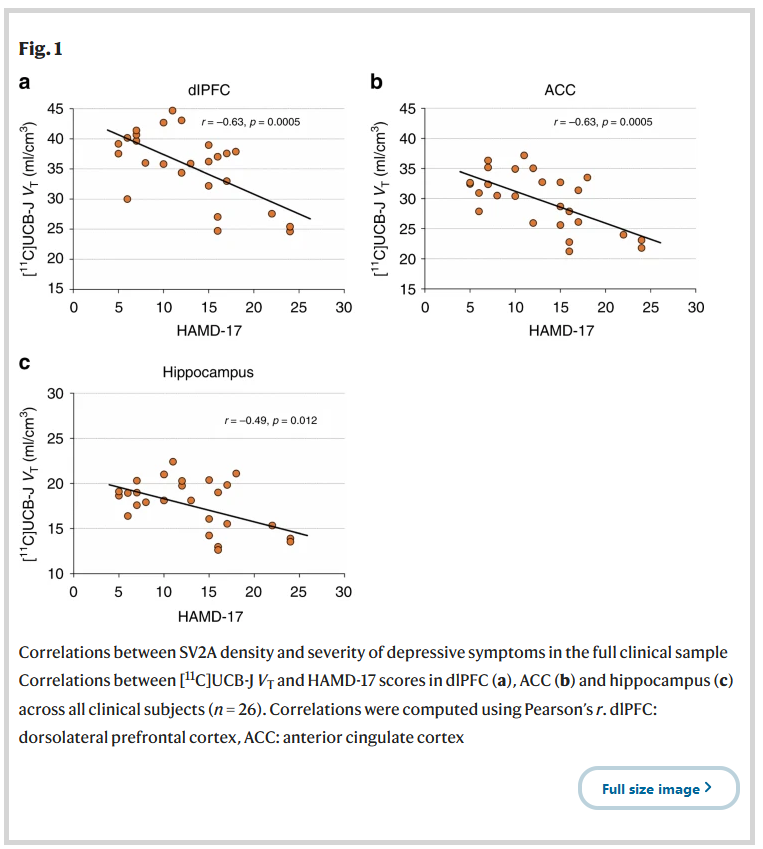 Source here. This is one of the least awful depression biomarkers I’ve ever seen
Source here. This is one of the least awful depression biomarkers I’ve ever seen
Put these two lines of research together and you get something like: synapse density increases over the course of the day, then sleep prunes it down again. Depression is associated with low synapse density. So it would make sense that depression gets better over the course of the day (including the extra-long artificial days of sleep deprivation) and then gets worse again after sleep.
Is this Rantamäki and Kohtala’s theory? I think their real theory is much more complicated than this and involves a bunch of different types of sleep, differential synapse density in various brain regions, and 24 pages of speculation about whether the effects of ketamine might change depending on what time of day you take it. One day I would like to quit my job, abandon all my friends, and spend six months in a cabin in Alaska trying to understand it in full. But I think this post is a decent first stab at an oversimplification. Here are a few subtopics I hope to eventually learn more about:
What is the role of REM vs. non-REM sleep? Depressed people have much more REM sleep than non-depressed people. Serotonin seems to decrease REM sleep, so unsurprisingly SSRI antidepressants decrease REM sleep a lot (not just in depressed people, in everybody). This would lend itself very nicely to a theory where REM sleep is involved in decreasing synapse strength, depressed people have too much of it, they end up with overly weak synapses, and that’s what depression is. In this model, antidepressants would treat depression by increasing serotonin levels in a way that represses REM. The problem with this is that in Tononi’s original paper, he says that the best evidence supports synaptic renormalization in non-REM sleep; he doesn’t have a great idea what REM is doing. He does mention one possibility is that non-REM sleep renormalizes most of the brain, but for some reason it doesn’t work on the hippocampus, and REM sleep renormalizes the hippocampus. And some of the studies on depression and synaptic density point to the hippocampus in particular. But others don’t, and this connection seems kind of forced. I think R&K mostly focus on slow-wave sleep and think it’s renormalizing incorrectly rather than just too much or too little.
How does this relate to TMS? Trans-cranial magnetic stimulation is a new-ish and exciting treatment for depression. You fire powerful magnets at the brain, which provokes neurons into firing. There’s some good evidence that this raises overall potentiation level, which I think is the same thing as synapse strength - and that it increases amount of sleep the next night, presumably to counterbalance this. But then how come, after being counterbalanced by sleep, it still has an effect?
How does this relate to electroconvulsive therapy? From Homeostatic Synaptic Plasticity Strategies In Neurological Disease:
Persistent changes in neuronal activity induce homeostatic compensation, which can manifest in numerous ways depending on the particular context. These mechanisms include alterations in the number, size and strength of synapses (homeostatic synaptic plasticity [HSP]) as well as a variety of other forms of regulating excitability. Chronic hypoactivity following seizures is predicted to induce homeostatic strengthening of excitatory synapses in order to restore network activity; a phenomenon that has been observed in some rodent seizure models.
That is, seizures seem to cause “strengthening of excitatory synapses”. Maybe this is why giving people seizures is such an effective depression treatment?
I’m having more trouble understanding R&K’s take on this. They write:
The administration of ECS [electroconvulsive shock] also produces prominent synaptic potentiation in rodents. Studies have shown that brief electroconvulsive seizures essentially reduce the degree to which further LTP can be induced in the dentate gyrus of anesthetized rats. Indeed, analyses of the EPSPs (excitatory postsynaptic potentials) and population spike size suggest that LTP induction had already occurred after ECS induced seizure activity,thus hampering further potentiation attempts (Stewart and Reid, 1993; Stewart et al., 1994). These results are also supported by a study in which hippocampal EPSP characteristics were monitored throughout a series of ECS treatments. The increase in EPSP slope developed gradually over the course of the first five seizures, whereas a single seizure did not induce a significant change (Stewart et al., 1994). The saturation of LTP-like plasticity and synaptic strength appears to resist further potentiation attempts, whereas weaker synapses are more likely to gain in strength.
So maybe it’s not just that seizures induce potentiation, it’s that they max out the strength of the strongest synapses, but keep adding more strength to the weaker synapses, meaning that renormalization increases the strength of weaker relative to stronger? So the overall result is to increase “equality” of synapse strengths throughout the affected regions? This sounds kind of like destroying information, but maybe if the information is the pattern of connections making you depressed that’s good?
How does this relate to circadian rhythm? We know disturbances of the circadian rhythm - when your body expects day vs. night - are heavily involved in depression, especially seasonal depression. We know circadian rhythm changes sleep architecture, altering the balance between REM vs. non-REM sleep. Is this why it has such a strong effect on depression? Maybe if we could figure this out we would have a better sense of whether it’s REM vs. non-REM sleep which is the issue here.
Bipolar disorder. If depression is related to decreased synaptic strength, is mania just increased synaptic strength? I can think of some reasons why it might be. In particular, sleep deprivation is a strong risk factor for mania. I think a good answer to this question would require me to understand the excitatory/inhibitory balance literature.
Relevance to the software : Elsewhere, I’ve reviewed a lot of promising cognitive theories for depression - ones that think of it as a global prior on negative stimuli, or abnormally low confidence on predictions, or something like that. That’s a pretty different approach from “decreased synaptic density in certain brain regions”.
I think everyone studying the brain operates on a model where some people will start at the hardware level and work up, other people will at the software level and work down, and hopefully they eventually meet in the middle. I still think that’s a good strategy.
How far are we? Is it fair to say that “decreased synaptic strength” is sort of the same thing as “abnormally low confidence on predictions”? If (to vastly oversimplify) my grandmother neuron has an abnormally weak synapse connecting it to my cake neuron, does that mean that I’m less able to believe confidently that my grandmother will give me cake? Does it mean that two hundred steps down the line in some kind of indirect way? Or is it more complicated than that, something like “your emotional system only has half as much RAM as usual today, so you’re not going to be able to trust anything you think”? Or is it something more like “your system for generating positive emotions only has half as much RAM as usual, but your system for generating negative emotions runs off a different sleep stage and is doing great, let’s go with that one”?
Overall I’m happy to have this extra framework, but it’s going to take a lot of work to fit the rest of the pieces together.