The Psychopharmacology Of The FTX Crash
Tyler Cowen linked Milky Eggs’ excellent overview of the FTX crash. I’m unqualified to comment on any of the financial or regulatory aspects. But it turns out there’s a psychopharmacology angle, which I am qualified to talk about, so let’s go.
I wrote this pretty rushed because it’s an evolving news story. Sorry if it’s less polished than usual.1
1: Was SBF Using A Medication That Can Cause Overspending And Compulsive Gambling As A Side Effect?
Probably yes, and maybe it could have had some small effect, but probably not as much as the people discussing it on Twitter think.
Milky Eggs reports a claim by an employee that Sam was on “a patch for designer stimulants that mainlined them into his blood to give him a constant buzz at all times”. This could be a hyperbolic description of Emsam, a patch form of the antidepressant/antiparkinsonian agent selegiline. The detectives at the @AutismCapital Twitter account found a photo of SBF, zoomed in on a scrap of paper on his desk, and recognized it as an Emsam wrapper.

Emsam is a brand of selegiline, a medication used since the 1960s to treat Parkinson’s disease. Selegiline is a MAOB inhibitor2. MAOB is an enzyme that breaks down dopamine3. If you inhibit it, you get more dopamine. So in a very broad sense, selegiline gives you more dopamine.4
Dopamine does many things in many brain systems. Here’s an oversimplified chart:
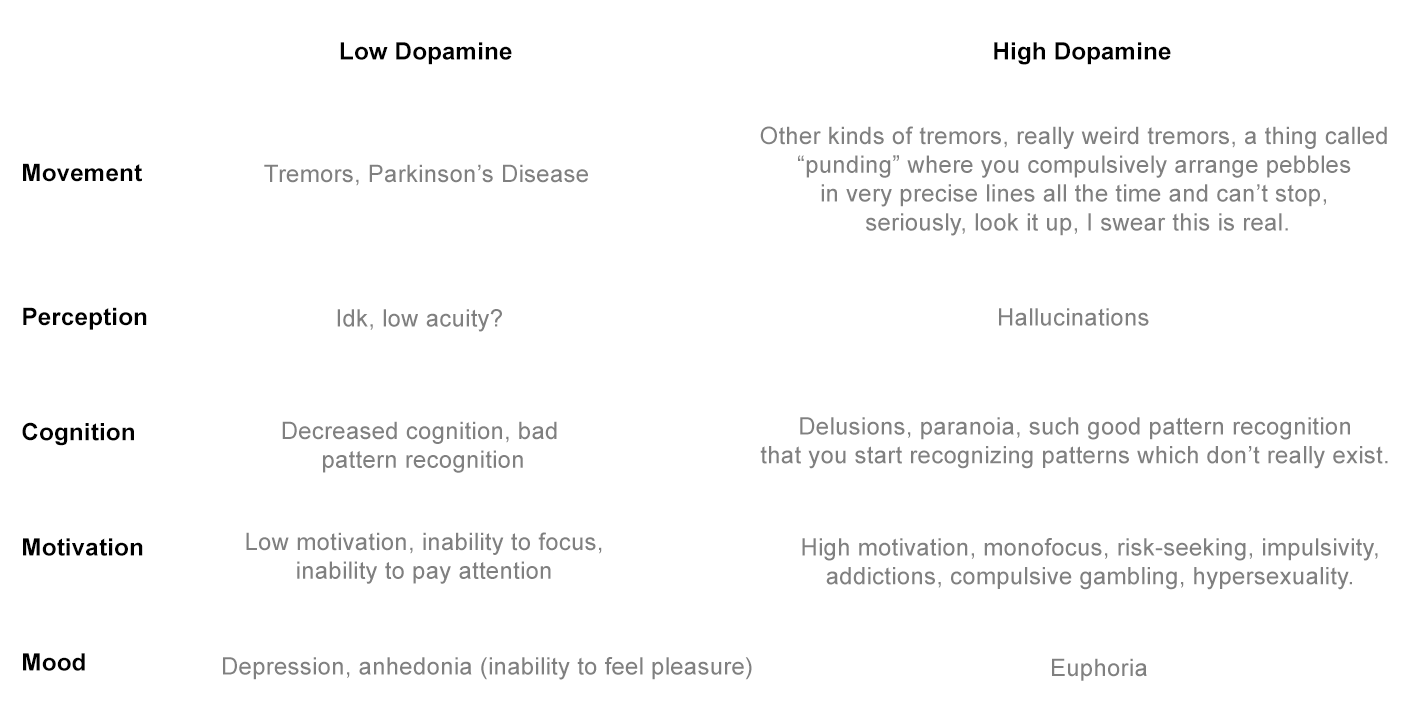
Everyone wants “magic bullets” - drugs that can increase dopamine in __ one of these ways, but not any of the others. Treat attention problems without causing hallucinations. Cure tremors without causing hypersexuality. But it’s tough. There are dozens of dopamine-based drugs, and all of them succeed in some ways and fail in others. Adderall mostly helps attention but sometimes causes a little paranoia on the side. Antipsychotics mostly prevent hallucinations and delusions, but also cause anhedonia. If a good doctor carefully chooses the right drug and dose, you’ll mostly get what you want. Otherwise, choose 2d4 random side effects from the appropriate side of the table.
Selegiline is an even less magical bullet than usual. People call it an antidepressant, anti-Parkinsonian, and stimulant, and all of those descriptions are accurate. It also does one unrelated thing: it disables a key digestive enzyme that prevents certain foods from killing you. For boring technical reasons, some pharma companies thought this might not happen if you delivered selegiline through a patch on the skin. For other boring technical reasons, the FDA disagreed and said people on the selegiline patch still shouldn’t eat those foods. The pharma companies decided to release the patch anyway, in case some people liked patches better than pills - and so Emsam was born.
Here’s what AutismCapital has to say about Emsam:
 Autism Capital 🧩 @AutismCapitalCommenters point out that EMSAM (Selegiline) has fatal effects if eaten with meat products. They also point out that it is linked to impulse control disorders such as pathological gambling and hypersexuality. This could explain Sam’s behaviour.
Autism Capital 🧩 @AutismCapitalCommenters point out that EMSAM (Selegiline) has fatal effects if eaten with meat products. They also point out that it is linked to impulse control disorders such as pathological gambling and hypersexuality. This could explain Sam’s behaviour. 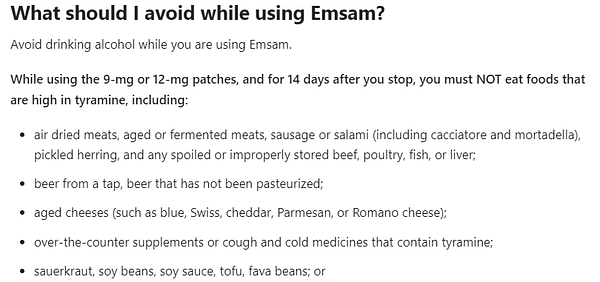
1,724Likes160Retweets](https://twitter.com/AutismCapital/status/1592256921813520385)
The “meat products” sentence is inexpertly phrased - as the link on the left explains, this is only true for certain dried meats like cured salami. And it’s equally true for some non-meat products like soy sauce. I’m only harping on this because some tweeters seized on this as a conspiratorial explanation for Sam’s vegetarianism, and that doesn’t make sense.
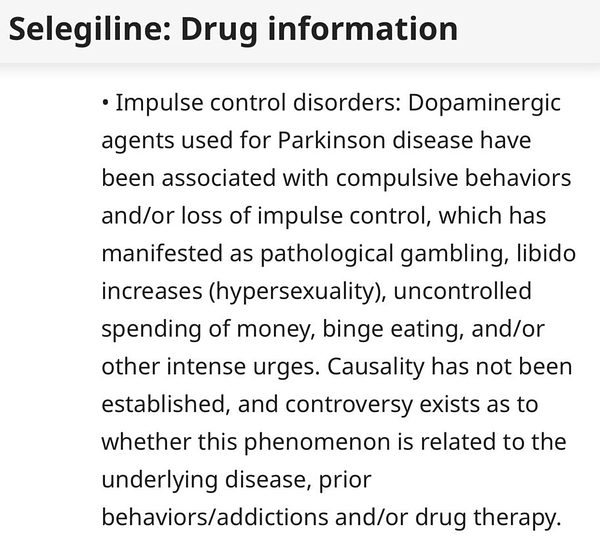
The pathological gambling is obviously more interesting. The link on the right quotes medicine.com, which says:
Dopaminergic agents used for Parkinson disease have been associated with compulsive behaviors and/or loss of impulse control, which has manifested as pathological gambling , libido increases (hypersexuality), uncontrolled spending of money , binge eating, and/or other intense urges. Causality has not been established, and controversy exists as to whether this phenomenon is related to the underlying disease, prior behaviors/addictions and/or drug therapy. Dose reduction or discontinuation of therapy has been reported to reverse these behaviors in some, but not all cases.
I can see why this caught so much attention. But let me rain on the parade: this seems pretty rare. Grossett et al found a prevalence of about 8% on any antiparkinsonian, but none of the 17 patients they found were taking selegiline. Lanteri et al quote a prevalence of 2.2 - 7%, but only one of the 15 patients they found was on selegiline, and that person was also on other medications more likely to cause the condition. This doesn’t prove that selegiline never causes problem gambling - but it suggests it’s one of the less likely medications to do so, probably at somewhere well below 2 - 8% of patients.
I was only able to find one case report of pathological gambling clearly caused by selegiline rather than some other medication - the fifth patient in Drapier et al (2006), which describes it as “the first case report in the literature”. And this definitely isn’t because doctors don’t like recording all the weird things selegiline can do - see eg the three case reports of selegiline causing transvestism (1, 2, 3)! 5
Does this mean that Emsam definitely wasn’t involved? Not exactly. “Gave someone a gambling disorder” is an overly binary way of saying “shifted someone’s brain’s risk curves6 a lot”. One of the case reports of antiparkinsonian-induced gambling was a “54-year-old, married pastor” who began gambling large sums daily after starting the pramipexole. It probably takes a lot of risk-curve-shifting to get a 54-year-old married pastor to go to Vegas and blow all of his savings. But if you’re already a cryptocurrency trader, maybe it only takes a tiny amount of risk-curve-shifting to turn you into a cryptocurrency trader who makes riskier trades. Maybe selegiline only shifts your risk curve a lot 0.001% of the time, but it shifts it a tiny bit more often than that.
Here’s a report by a Wall Street trader who got addicted to cocaine - another dopaminergic drug:
It’s not like you rip one line and then all of a sudden your life falls apart. For me, I started to have what I thought was more fun at night, which resulted in less success during the day. I was still making money, but not making great decisions all of the time. My formula for success started slipping away from me. It took about two whole years before the wheels started to fall off. Then I started losing money and making very poor choices in and out of the office.
During my years of struggling with addiction, my trading suffered. One of my first seven-figure losses came because I’d lost focus and attention to detail. I just didn’t do the clerical part of my job over options expiration. And when I came into work on Monday, I learned that it cost our firm over a million dollars. And in 2009, I lost hundreds of thousands of dollars personally. I was stubborn. I was adamant that the market shouldn’t be rallying as much as it was. I was short, stayed short and doubled down. And the entire time I knew I was breaking a cardinal rule of trading: Don’t fight the Fed.
I don’t think Emsam is vastly worse than other dopaminergic drugs - maybe even including common drugs like Adderall. I think all of these drugs are fine for ordinary people who need antidepressants or stimulants. They might even potentially be fine for people who work with risk as a job, like traders - especially if they’re following an algorithm or having their work checked by other people. But if someone’s making big decisions based on their intuitive risk assessments, they should keep in mind that dopaminergic drugs can shift the way they think about those things - not necessarily to a worse place, just a different place.
A significant fraction of the finance industry is on Adderall - I know because they keep trying to make me prescribe it to them. This hasn’t degraded performance so much that managers have noticed or made rules against it. And for all I know, maybe the medicated mental risk curves are better for trading than the unmedicated ones. Still, I would warn everyone involved to be careful.
2. Is There Some Conspiracy That His Name Was Sam And He Was On A Medication Called Emsam?
This is a surprisingly popular question on Twitter by people who I assume are trolling but you never really know:
 beleth @3elethEmsam was the MAOI Sam used. Why is no one questioning why the drug has his FIRST NAME in it?? How deep does this really go?[3:09 PM ∙ Nov 12, 2022
beleth @3elethEmsam was the MAOI Sam used. Why is no one questioning why the drug has his FIRST NAME in it?? How deep does this really go?[3:09 PM ∙ Nov 12, 2022
3Likes1Retweet](https://twitter.com/3eleth/status/1591448204415229953)
 Lucre Snooker @LucreSnooker@soncharm wait hang on the rumored drug is brand-name “Emsam” Emsam = EM + Sam Elon Musk + Sam 😨11:06 PM ∙ Nov 14, 2022
Lucre Snooker @LucreSnooker@soncharm wait hang on the rumored drug is brand-name “Emsam” Emsam = EM + Sam Elon Musk + Sam 😨11:06 PM ∙ Nov 14, 2022
Emsam is in fact named after the two kids of the CEO of the pharma company that developed it: Emily and Sam. This is the cutest psychopharmacology fact I know.
3: What Was In The Blue-Green Bottle?
Going back to @AutismCapital’s picture:
What’s the blue-green bottle to the left of the red circle?
Here the detectives on r/NootropicsDepot recognized it as their company’s old brand of adrafinil7. Adrafinil is a prodrug of modafinil, an unusual stimulant-like drug. That is, your body metabolizes adrafinil and turns it into modafinil after you take it.
So was SBF effectively on modafinil? Seems likely - many traders are. I won’t lie - modafinil is a good stimulant, during medical residency some doctors (including me) would use it to stay alert through the night shift. It’s not any better than Adderall or anything, just a bit different and easier to get.
Does it affect attitudes to risk? Hopefully you can already predict my answer to that question: all dopaminergics affect attitude to risk in complicated ways we don’t really understand, but for most people these effects will be too small to notice. There’s one case report of modafinil causing pathological gambling, and various contrived studies where neuroscientists investigate how modafinil shifts some technical parameter in a risk curve; these kinds of studies often don’t replicate. I think you can really just stick to your prior of “all dopaminergics affect risk curves in ways we don’t understand, but it’s usually fine when your job doesn’t require perfectly-tuned risk awareness”.
Except - was he taking the selegiline and adrafinil at the same time?
Selegiline prevents the body from breaking down dopamine. Modafinil works by preventing cells from reabsorbing dopamine. If you can’t break it down, and you can’t reabsorb it, what happens? Does it just build up forever until it explodes and you die?
This is what happens with serotonin. If you take a drug that prevents serotonin breakdown (like a traditional MAOI) and a drug that prevents serotonin reuptake (like an SSRI) at the same time, you definitely die. Lots of doctors have noticed that the MAOI + stimulant situation is pretty similar and decided you shouldn’t take these at the same time either. So some people following the FTX situation have wondered whether this combo might have been very dangerous - either to Sam’s health or to his risk-management ability.
 Phirrrr @phirrrrTaking Emsam by itself - not going to do much. Taking Emsam and amphetamines - can send you to the hospital feeling like your heart is about to explode. In general I would not abuse Emsam, MAO drugs generally pretty intense. Probably treats major depression effectively though.
Phirrrr @phirrrrTaking Emsam by itself - not going to do much. Taking Emsam and amphetamines - can send you to the hospital feeling like your heart is about to explode. In general I would not abuse Emsam, MAO drugs generally pretty intense. Probably treats major depression effectively though.  Autism Capital 🧩 @AutismCapitalWe’ve received confirmation that Sam’s drug was actually Emsam. It is a drug normally used to treat Depression and Parkinson’s disease but also gives performance enhancing and wakefulness effects. https://t.co/F5iAwZaCrc12:07 PM ∙ Nov 12, 2022
Autism Capital 🧩 @AutismCapitalWe’ve received confirmation that Sam’s drug was actually Emsam. It is a drug normally used to treat Depression and Parkinson’s disease but also gives performance enhancing and wakefulness effects. https://t.co/F5iAwZaCrc12:07 PM ∙ Nov 12, 2022
My verdict: this is a bad idea but - surprisingly! - probably won’t literally kill you.
MAOI expert Dr. Ken Gillman writes about MAOIs and amphetamines, but I think the lessons more or less carry over to MAOIs and modafinil:
One or two recent papers about the mechanisms of action of MAOIs and amphetamine at the molecular level suggest why the combination of amphetamine (with MAOIs) is not unduly risky as has been (mis)stated for so long. Care and experience are required but it can be done safely although small increases in dose do sometimes seem to have disproportionate effects.
There is now quite a lot of accumulated experience of the concurrent administration of MAOIs and amphetamine for therapeutic purposes in depression. It is safe when done carefully. Early concerns about frequent hypertension have not materialized and recent clinical reviews indicate judicious use is safe (21, 22). Since amphetamine is substantially more potent than ephedrine it would seem, by extension, that concerns over this drug may also have been be over-rated. If taken in supra-therapeutic doses or overdose the situation may be different.
Also, Israel 2015, Combining Stimulants and Monoamine Oxidase Inhibitors: A Reexamination of the Literature and a Report of a New Treatment Combination follows a patient who took selegiline and lisdexamfetamine at the same time, notes with surprise that they didn’t die, and concludes that:
The present case adds to the literature describing effective combinations of MAOIs and stimulants and suggests that the combination of transdermal selegiline and a stimulant may not need to be considered absolutely contraindicated. This combination therapy may be an option for some patients with comorbid ADHD and treatment-resistant MDD when used with caution and monitoring of heart rate and blood pressure.
Based on reports like these, I once placed one patient, one time, on a combination of MAOIs and amphetamines, during a situation where I thought potential benefits outweighed risks. I quadruple-checked every detail of the regimen, prayed, and added my malpractice attorney’s phone number to speed dial. In the end it went fine. But it’s not a combination I would recommend trying at home.
Even it’s not deadly, could a MAOI + stimulant shift risk-sensitivity even more than selegiline or modafinil alone?
Again, my answer is going to be “all dopaminergics shift risk-sensitivity, usually to relatively small degrees, but maybe enough that it would become relevant in an unusual situation like crypto trading”. Would this unusual interaction do it more than usual? Maybe, hard to say, but my wild guess is probably not - for example, in this study, the addition of selegiline didn’t make people feel any higher on cocaine.
Also, I don’t even know if SBF was really taking these at the same time. There was just a photo with (what looked like) both of them on his desk.
4: Was Everyone On Meth?
Get ready for a galaxy-brained answer here: Nobody took meth. Nobody thought they were on meth. But in fact they were on meth. But actually it’s fine and you don’t need to worry.
Backing up: for some reason, a bunch of crypto accounts are assuming meth was involved:
 foobar @0xfoobarFTX is a sex cult and secret hedge fund that paid off congress to ban their competition and gambled away everyone’s deposits while high on meth the worst part? my paid group TA predicted everything[11:26 PM ∙ Nov 10, 2022
foobar @0xfoobarFTX is a sex cult and secret hedge fund that paid off congress to ban their competition and gambled away everyone’s deposits while high on meth the worst part? my paid group TA predicted everything[11:26 PM ∙ Nov 10, 2022
2,337Likes184Retweets](https://twitter.com/0xfoobar/status/1590848474299662339)
As far as I can tell, nobody has evidence beyond this tweet by the Alameda CEO:
 Caroline @carolinecapitalnothing like regular amphetamine use to make you appreciate how dumb a lot of normal, non-medicated human experience is[11:41 AM ∙ Apr 5, 2021
Caroline @carolinecapitalnothing like regular amphetamine use to make you appreciate how dumb a lot of normal, non-medicated human experience is[11:41 AM ∙ Apr 5, 2021
1,995Likes518Retweets](https://twitter.com/carolinecapital/status/1379036346300305408)
…which seems pretty obviously about normal amphetamine (ie Adderall) rather than methamphetamine. For example, she’s describing it as “regular” and “medicated”. And admitting it publicly while being the CEO of a major company. Also, 99% of amphetamine users are on Adderall and not meth. Come on!
But , as I said before, unrelated to this, at least some of them were in fact on meth.
See Romberg 1995, Methamphetamine and amphetamine derived from the metabolism of selegiline. When you take selegiline, your body metabolizes it into other chemicals. One of them is methamphetamine. How much? Probably lower than the levels methheads get, but maybe around the threshold for being clinically relevant.
Luckily for them, this is l-methamphetamine, the mostly-inactive stereoisomer of meth (if you don’t know what stereoisomers are - do you know how all superheroes have an evil version of themselves with a goatee from a parallel universe? This is that, but for organic chemicals). There’s boring technical debate about exactly how dangerous and addictive l-methamphetamine is, but the answer I find most convincing is “so safe and nonaddictive that the government lets you sell it over the counter as a nasal decongestant”
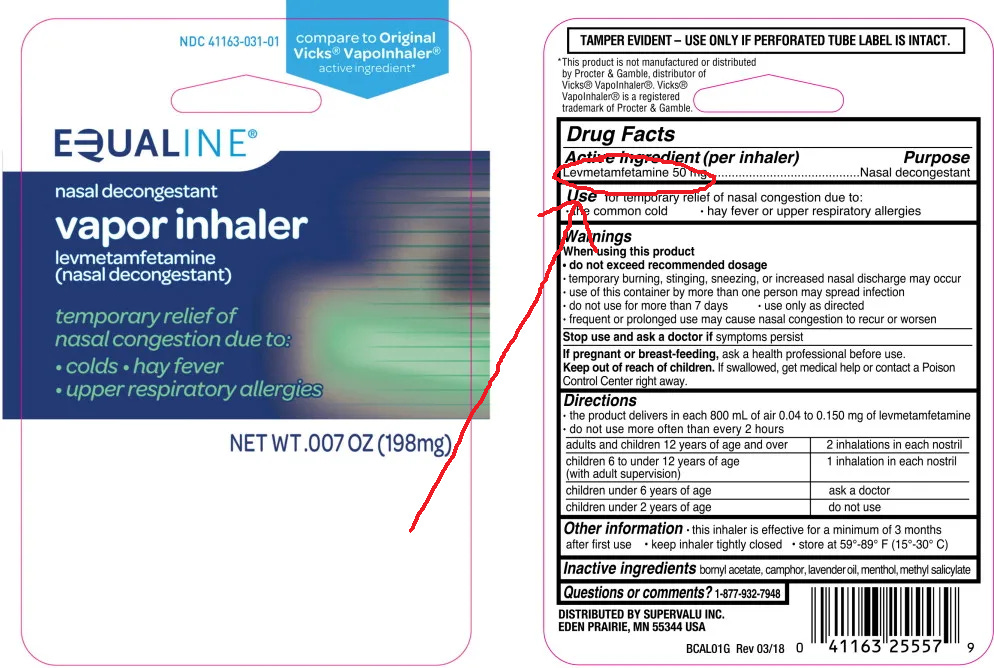 The government also lets you spell it “levmetamfetamine” on the ingredient list so people don’t see it and freak out.
The government also lets you spell it “levmetamfetamine” on the ingredient list so people don’t see it and freak out.
Anyone taking selegiline might get a positive urine test for methamphetamine, but there’s no reason to expect any real negative effects.
5: Okay, But Was Everyone On Other Stimulants?
An account posted on AutismCapital says:
The NYT interviews the psychiatrist, who denies that stimulants were overused:
I originally wrote here that “In line with most tech companies” was a great euphemism for “yes, we were overusing stimulants”. But many commenters responded that they’re in tech, and neither they nor most of their friends take stimulants. So I think this was overly hasty of me.
Probably it’s selection bias - as a Bay Area psychiatrist, I see the people who are in stimulants, but not the ones who aren’t. A few years ago I wrote a piece on my experience as working in SF’s business district:
The human brain wasn’t built for accounting or software engineering. A few lucky people can do these things ten hours a day, every day, with a smile. The rest of us start fidgeting and checking our cell phone somewhere around the thirty minute mark. I work near the financial district of a big city, so every day a new Senior Regional Manipulator Of Tiny Numbers comes in and tells me that his brain must be broken because he can’t sit still and manipulate tiny numbers as much as he wants. How come this is so hard for him, when all of his colleagues can work so diligently?
(it’s because his colleagues are all on Adderall already – but telling him that will just make things worse)
He goes on to give me his story about how he’s at risk of getting fired from his Senior Regional Manipulator Of Tiny Numbers position, and at this rate he’s never going to get the promotion to Vice President Of Staring At Giant Spreadsheets, so do I think I can give him some Adderall to help him through?
Psychiatric guidelines are very clear on this point: only give Adderall to people who “genuinely” “have” “ADHD”.
But “ability to concentrate” is a normally distributed trait, like IQ. We draw a line at some point on the far left of the bell curve and tell the people on the far side that they’ve “got” “the disease” of “ADHD”. This isn’t just me saying this. It’s the neurostructural literature, the the genetics literature, a bunch of other studies, and the the Consensus Conference On ADHD. This doesn’t mean ADHD is “just laziness” or “isn’t biological” – of course it’s biological! Height is biological! But that doesn’t mean the world is divided into two natural categories of “healthy people” and “people who have Height Deficiency Syndrome“. Attention is the same way. Some people really do have poor concentration, they suffer a lot from it, and it’s not their fault. They just don’t form a discrete population […]
We could still have a principled definition of ADHD. It would be something like “People below the Nth percentile in ability to concentrate.” Instead, we use the DSM, which advises us to diagnose people with ADHD if they say they have at least five symptoms from a list. The list has things like “often has difficulty sustaining attention” and “often has difficulty organizing tasks”. How often? You know, often! And if you work as a Senior Regional Manipulator Of Tiny Numbers, you’re going to have attention problems a lot more “often” than the rest of us.
ADHD is so poorly defined that the official standards basically boil down to “it’s hard to do your job without Adderall”. Coding takes a lot of focus, and it’s hard to do without Adderall for a lot of people. I want to back off from saying it’s omnipresent, because commenters are telling me it’s not, but I’d be interested in finding firm numbers. See my original piece on Adderall for more thoughts on this.
At normal doses, most people can think clearly on stimulants; unless there was some evidence of abnormal doses or missed sleep (see below) I usually wouldn’t expect this to have a clinically significant effect on judgment. But again, if it showed up anywhere it would show up in complicated trading.
6: Is It Okay, As A Psychiatrist Bound By Doctor-Patient Confidentiality, To Give An Interview About Your Patient To The New York Times?
What? No!!! Obviously not!!! Why would you even ask this question? What the heck?
This isn’t really a psychopharmacology question. And yet in answering the last psychopharmacology questions, I did end up having to read FTX’s In-House Performance Coach Is Just as Surprised as You Are. Apparently the FTX company psychiatrist gave an interview to the New York Times on his opinion of SBF’s personality.
He claims this is okay, because he was just a “performance coach” for the company, who happened to, additionally, be a psychiatrist who was treating many of the company’s employees. This is not better. Psychiatric ethics tries to have careful conflict-of-interest rules so that you aren’t playing multiple roles for the same person. For example, suppose you are employed as a “performance coach” in the Bahamas by a famously generous and free-spending company. And suppose that company has made it extremely clear that they want their employees to be on stimulants. And suppose you are treating those employees, and need to decide whether to put them on stimulants or not. It seems kind of plausible that maybe if you didn’t give the employees stimulants, you would lose your cushy Bahamas job. Isn’t this going to unduly influence your prescribing decisions?
I’m usually the last person to be a stickler for role-conflict-rules - I prescribe to family members in emergencies, and sometimes the emergency is “they are bad at getting a real doctor”. But this is just way beyond anything that even I would consider appropriate.
And even aside from that, it’s just crazy for any kind of a mental health professional to give an interview to the New York Times about anyone in an even slightly patient-like capacity. Even supposing that he wasn’t SBF’s psychiatrist (but then who was prescribing the Emsam?) this violates a norm against psychiatrists publicly assessing famous figures8. I suppose Dr. Lerner will argue that he was assessing Sam with his performance coach hat rather than his psychiatrist hat - no guessing how many FTT tokens I think that distinction is worth.
But aside from that, really? REALLY? When the New York Times , for its own stupid reasons, tried to write an article that would compromise my ability to avoid a weird multiple-role-conflict with my patients, I quit my job and tried to contribute what little I could to the ongoing campaign of all reasonable people to destroy the New York Times. This was the correct, ethical thing to do! And he just . . . voluntarily offered them an interview? About his patient performance coachee? REALLY?
I’d like to think that maybe SBF asked him to do this interview and gave 100% express consent. But even then, there’s a marit ayin consideration - the psychiatrist should start by very explicitly saying he has express consent, and would never do anything like this without it.
The best I can say for him is that he’ll probably get away with it, because the only injured party is Sam Bankman-Fried, and I assume Sam’s lawyers are busy right now.
7: So Was This All Because Of Weird Drugs?
I don’t really want to have an opinion on this, because I assume at some point one of their lawyers will hit on the defense “it was all because of weird drugs”, and I don’t want to seem like I’m shilling for one side or the other in a legal case.
I think you could make an argument that dopaminergic drugs shift various complicated risk curves in the brain. But a lot of Wall Street is on stimulants of one sort or another, and most of them don’t act like FTX did. Emsam is a little stranger than the usual Wall Street stimulants, and combining it with other stimulants might amplify the effects. But I still would think in terms of “how much are we moving the risk curves, and is it really that much further than a lot of other things do all the time?” rather than “does this switch you into uncontrollable pathological gambling mode?”
If I were one of the psychiatrists who will one day buy second houses from the money they make as expert witnesses on this case (DON’T EVEN THINK ABOUT ASKING ME TO DO THIS9), I would focus on what doses were involved. Adderall 10 mg will help treat ADHD and give you a nice motivational boost. Adderall 200 mg will cause paranoia and sometimes hallucinations. There are similar considerations for modafinil and Emsam. All of these drugs are compatible with “probably didn’t matter” or “probably the main cause of everything” depending on what doses we’re talking about.
(and of course there could be other drugs I don’t know about)
The other free advice I would give these witnesses is to think about sleep. The most common way stimulants cause psychosis (this is my personal opinion, I haven’t checked if the literature agrees with me) isn’t by some kind of direct dopaminergic agonism. It’s by making it feel possible to operate on two hours of sleep a night. This is not actually possible and will land you into some kind of very exotic and maladaptive mental state. Someone who takes lots of stimulants during the day and then manages to sleep fine at night might do better than someone who takes the same amount of stimulants in order to work 130 hour weeks.
Free advice to the rest of you: I described certain drugs here as relatively safe, or potentially useful, but I want to emphasize that these are all serious medications and you shouldn’t mess with them lightly. Modafinil is great - except that it might cause fatal skin rashes in young people, it can break birth control, etc. Emsam is fine, except that it will kill you if you eat certain types of cheese, etc. I’m providing you with infotainment, not the much longer and more warning-filled lecture I would give to people who I was actually prescribing these to. Please don’t rush out to abuse drugs just because you read about them in an article on how they contributed to a $10 billion bankruptcy.
Footnotes
HAHAHAHAHAHAHAHAHAHA. Holy fucking shit! I just looked him up. Totally a customer of ours… Crypto Bernie Madoff was our customer. LOL
What a fucking asshole! Illegally stealing customer’s deposits to gamble on shitcoins through his Alameda Research fund! He’s the reason BTC was depressed this bull cycle. Sam is the reason I am still here watching fucking depressing crypto news instead of being completely out and having lower blood pressure… and he is a fucking customer of ours! What a weird fucking world this is.
LET ME REPEAT THIS FOR EVERYONE AGAIN: Shitcoins are bad, and you should feel bad if you trade them. Get the fuck out of the shitcoin casino you dumb ass gamblers! Solana is garbage. TRON is garbage. Exchanged-based coins like FTT are garbage. Coins with fucking dogs faces are garbage. Bitcoin is the only cryptocurrency you should hold. Maybe ETH. Hedge your bets there. You need to CONTROL YOUR OWN KEYS. Don’t lend your coins out to charlatans promising you 5%, 8%, 15%, or 20% “risk free” returns. They are all scam Ponzis. There is no such thing as risk free 20% returns. It doesn’t exist. Stop chasing it. If you don’t control your private keys, it’s not your crypto. If you trust an exchange based in the Bahamas ran by a jabroni who thinks he needs SIX MONITORS, you are in for a bad time. I’ve been in cryptocurrency since 2010 when BTC was 81 cents. I lived through the MT GOX implosion. I have had more crypto stolen from me in hacks and exit scams than you probably have ever even seen. Learn from my experience. Listen to what I am saying. TWELVE YEARS now I have been in crypto. This too shall pass. Fuck all these frauds stealing everyone’s shit. We will all be better off with them out of the industry. However, you all have to learn from this shit. CONTROL YOUR OWN KEYS! Stop gambling on shitcoins. You are being used as exit liquidity for idiots.
The reason cryptocurrency has changed the world, and will continue changing the world, is not because a fucking Shiba inu coin went 10,000%X because a narcissistic man-baby tweeted about it. It’s because decentralized sound money has value. I’ve seen crypto build up from literally nothing. Even buying bitcoin was next to impossible back then. I mined BTC with my laptop at first. I stopped because I “only” mined 5 BTC per night, and it was using too much power. My first BTC I ever bought was when I met a fat dude wearing a Super Mario Brothers T-shirt at Home Depot. We met in the garden section and sat on a bench to talk about how bitcoin worked, how it was going to change the world, and how to transfer between wallets. I still have the wallet I setup and used to buy that BTC from him. Through all the craziness that has happened in the crypto space over the past 12 years, I have always been able to access my private wallets. Store your crypto in your own cold storage wallet unless you are actively trading. The moment you “lend” your coins out to someone for yields, it’s already as good as gone. You’ve missed the entire point that Satoshi tried to get across so many years ago. Not your keys, not your coins. If you lost money in this shitshow, don’t worry. This will all pass, and we will all be stronger for it. Just learn from it all and move on. Buy BTC and ETH, hold it in your cold storage wallets, and wait for the next bull cycle. Watch out for thieves and frauds trying to convince you into “the next big coin.” They are all liars and thieves. Real cryptocurrency will endure. For it to really flourish, the shitcoin casinos must die. If you buy some new fucking Frodo Baggins faced shitcoin in the future and lose it all, you only have yourself to blame.
I never wanted to still be sitting here watching all this crypto drama, but people like SBF fucked this cycle up. I feel everyone’s pain. I’ve lived through many crashes now. I am more dead inside than I was, but it is never easy to watch shit crash. If you want real sound crypto, you have some good buying opportunities here. Mid 2024 we will go through the ups again. Ignore all the morons saying this time is the end. I’ve heard that every crash since 2010. The next time we hit the bull market, stick to sound crypto projects and control your own private keys. Don’t let frauds like SBF have your coins. You control your crypto, or you don’t own it.
The patient’s lawyer got to cross-examine me. He decided to die on the hill of “the patient never really drank the bleach”. He pointed out that the patient had been admitted directly to the psychiatric hospital without spending any time in a medical hospital, and asked me if it was realistic that someone could drink bleach and not have to spend time in the hospital.
I’m not a toxicologist and I didn’t know the details of bleach poisoning. But I also felt like I was up there as this supposedly expert doctor and it would be humiliating not to know this basic fact. But also I was under oath and not supposed to lie. So I mumbled something about how, I don’t know, drinking bleach seems bad but maybe you don’t always end up critically ill and in the hospital, I don’t know, can we please move on.
The defense attorney got really angry and asked “Well, have YOU ever drunk bleach, Dr. Alexander?” My hospital’s lawyer objected, and the defense lawyer said some legal stuff, and the two of them argued about it for a second, and finally the judge indicated that she would allow the question and I had to tell the court whether I had ever drunk bleach.
I had to admit I had not.
The defense attorney asked, still pretty condescendingly, whether this was because, without any medical expertise, using my total layman common sense, I thought that drinking bleach was probably really bad and would land you in the hospital or something.
I was kind of panicking, and I didn’t know what to do, and I worried I had just destroyed all my credibility as a doctor by not being able to emphatically say that drinking bleach required immediate hospitalization, and now I didn’t know whether I was going to look like I was walking back on my previous statement or what, so I just answered that yes, drawing on all of my expertise and years of training, all I could do was tentatively conclude that it seemed like, on net, drinking bleach was probably worse than not doing that.
The defense attorney got very excited, like I had just conceded the whole case. Then he asked me a lot more questions, and I must have handled them okay because the judge eventually gave our side the commitment order they wanted.
Then I went home and immediately Googled “how bad is drinking bleach”, and according to this site:
Should you worry about drinking a mouthful of bleach? You’ll probably be fine. Most household bleaches contain fairly low concentrations of sodium hypochlorite – about 3 to 6 percent. That’s not an endorsement for trying it, but for the average adult, you shouldn’t expect anything worse than an upset stomach.
HE WAS JUST BULL$#!TTING THE WHOLE TIME!
This is why I will never again be an expert witness no matter how much they offer to pay me.
-
Conflict of interest notices: I was friends with an FTX/Alameda employee a few years ago. I support the effective altruist movement, which FTX donated money to. I briefly worked at the same San Francisco clinic as Dr. Lerner, a psychiatrist mentioned in this piece - but I’m so introverted at work that I never actually met him.
-
There are many boring technical details about at what doses it is a MAO-B vs. MAO-A inhibitor; please forgive me for not mentioning them here.
-
In the process of double-checking this, I came across this article from last year which says we’ve been understanding MAOB all wrong for decades and everything works differently than we think. I haven’t fully absorbed it yet, but you could combine this with a story where selegiline exerts its stimulating dopaminergic effects through its amphetamine metabolites. I’m going to stick to the textbook explanation in the main article so I don’t have to have an opinion on this.
-
I’m trying to write a rushed article about breaking news, please forgive me for writing sentences like these instead of linking to two thousand pharmacology papers about the thing these sentences are oversimplifications of.
-
I’m sorry to use the old offensive terminology, but I do so deliberately here. These studies were done decades ago, when nobody had heard of transgenderism, and when “transvestism” was considered incredibly shameful. I don’t think these drugs were changing people’s gender identity. I think these patients were probably repressing pre-existing desires about gender nonconformity, the drugs made them more risk-seeking, and so the patients made the risky decision to express their gender issues in the (socially dangerous) way available to them at the time. All of this probably has Vast Societal Implications.
-
I’m using this awkward term “risk curves” to refer to a bunch of neuroeconomic concepts I only vaguely understand, sorry.
-
The head of Nootropics Depot, MisterYouAreSoDumb, made a comment on the situation, which I reprint here in its entirety:
-
Some commenters ask if this article you’re reading now also breaks that rule. I’d like to think no - I think it permits talking about larger concepts (like what the side effects of different medications are) as long as you avoid individuals’ personalities. I admit that other people may be less invested in that distinction than I am.
-
Fine, since you’ve read this far, here’s the story of the last time I had to testify in court as an expert witness, slightly amended from some old notes I wrote at the time, way back when I was a resident. The only fact I will give you about the patient is that they drunk bleach as a suicide attempt, which describes some significant fraction of all psychiatric inpatients, so I don’t think it’s a confidentiality violation. I had been conscripted into representing my hospital, which was trying to get a longer involuntary commitment order.